Multi-Organ Involvement of an Immunoglobulin G4-Related Inflammatory Pseudotumor of the Urogenital Tract: A Case Report
- Affiliations
-
- 1Department of Radiology, Eulji Hospital, Eulji University School of Medicine, Seoul, Korea. jyy@eulji.ac.kr
- 2Department of Pathology, Eulji Hospital, Eulji University School of Medicine, Seoul, Korea.
- 3Department of Urology, Eulji Hospital, Eulji University School of Medicine, Seoul, Korea.
- KMID: 2130950
- DOI: http://doi.org/10.3348/jksr.2015.73.6.418
Abstract
- Inflammatory pseudotumor (IPT) is a rare solid tumor of unknown etiology that can arise in most organs. IPT usually presents as a single, benign lesion. In the urogenital tract, IPT frequently occurs in the bladder, but in rare instances, IPT may originate in the kidney, prostate, or ureter. We describe a highly unusual case of multi-organ IPT that included the periureteral area, paravesical space, and prostate. The diagnosis was confirmed by computed tomography imaging, and by pathology testing that detected prominent immunoglobulin G4-positive plasma cells.
MeSH Terms
Figure
-
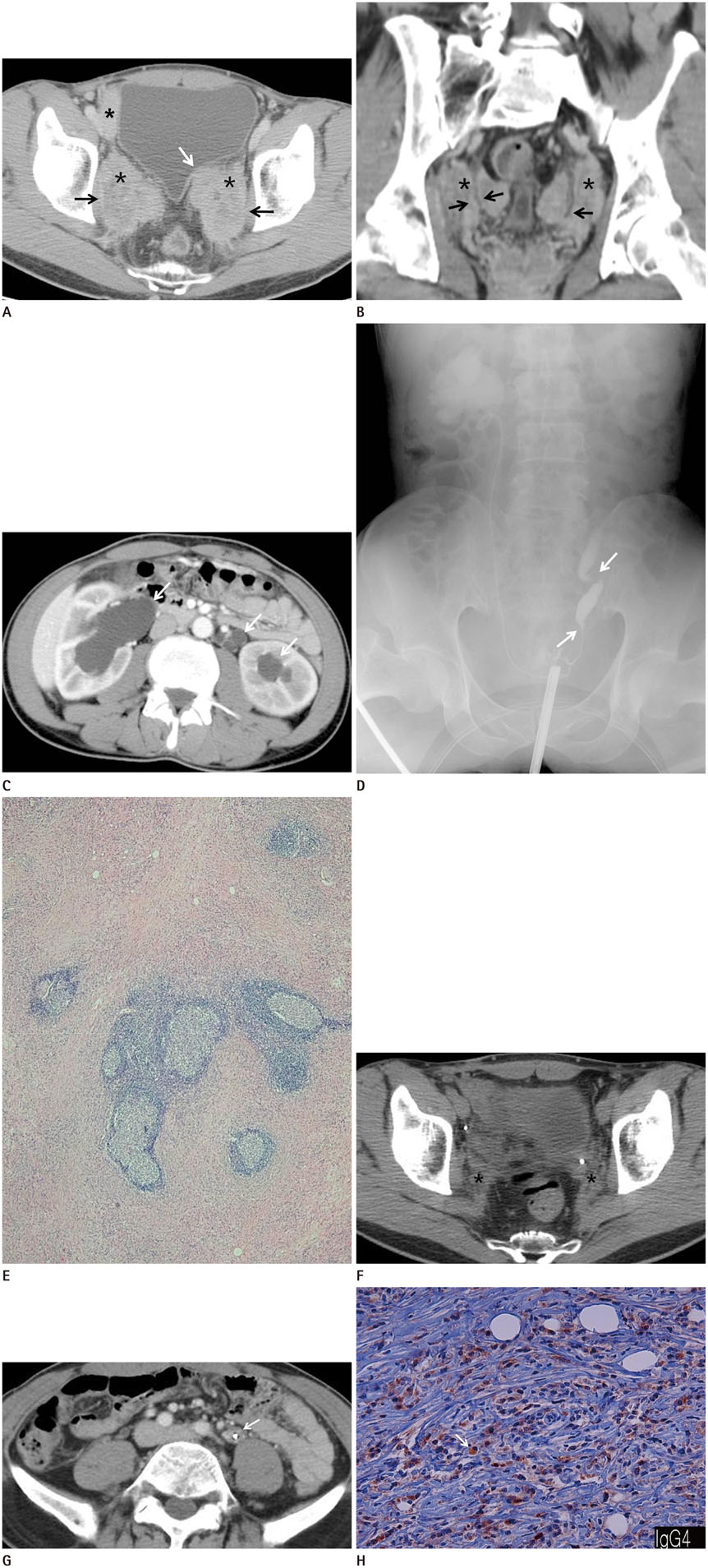
Fig. 1 A 50-year-old man with multi-organ involvement of IgG4-related inflammatory pseudotumor of the urogenital tract. A. Axial contrast-enhanced CT image showing three ill-defined heterogeneous, delayed enhancing masses in the right paravesical space and bilateral periureteral areas (asterisks). Each bilateral periureteral mass encases a distal ureter, and the left periureteral mass abuts the inferior bladder wall (white arrow). Infiltration of the bilateral obturator muscles is shown (black arrows). B. Coronal reformatted contrast-enhanced CT image showing bilateral periureteral masses (asterisks) and irregular wall thickening and luminal narrowing of the bilateral distal ureters (black arrows) from tumor involvement. C. Axial contrast-enhanced CT image demonstrating bilateral hydroureteronephrosis (arrows). D. Retrograde pyelography image showing right hydronephrosis with double-J catheter insertion in the right ureter, and segmental dilatation and stenosis (arrows) of the left distal ureter. IgG4 = immunoglobulin G4 E. Microscopic photomicrography of the paravesical mass showing spindle cell proliferation with diffuse marked fibrosis, accompanying marked infiltration of plasma cells, lymphocytes, histiocytes, and eosinophils with lymphoid follicles (hematoxylin and eosin stain, × 100). F. A follow-up axial contrast-enhanced CT scan after surgery, radiation therapy, and steroid hormone therapy, showing marked decreases in the size of the bilateral periureteral masses (asterisks). G. The last follow-up axial contrast-enhanced CT image revealing a soft tissue lesion encasing the left proximal ureter (arrow). H. The additional immunohistochemistry stain on high power field microscopy performed after suspicion of IgG4-related IPT, showing a high volume of IgG4-positive plasma cells (arrow). IgG4 = immunoglobulin G4, IPT = inflammatory pseudotumor
Reference
-
1. Harper L, Michel JL, Riviere JP, Alsawhi A, De Napoli-Cocci S. Inflammatory pseudotumor of the ureter. J Pediatr Surg. 2005; 40:597–599.2. Lee JW, Kim KW, Paek KM, Park MS, Seok JY, Kim S, et al. Non-contiguous multi-organ involvement of an inflammatory myofibroblastic tumor: a case report. J Korean Radiol Soc. 2007; 57:265–269.3. Kim SA, Lee SR, Huh J, Shen SS, Ro JY. IgG4-associated inflammatory pseudotumor of ureter: clinicopathologic and immunohistochemical study of 3 cases. Hum Pathol. 2011; 42:1178–1184.4. Kim H, Oh SN, Rha SE, Jung SE, Lee YJ, Byun JY, et al. Inflammatory myofibroblastic tumor of the bladder: report of two cases. J Korean Soc Radiol. 2010; 63:261–265.5. Ryu KH, Im CM, Kim MK, Kwon D, Park K, Ryu SB, et al. Inflammatory myofibroblastic tumor of the kidney misdiagnosed as renal cell carcinoma. J Korean Med Sci. 2010; 25:330–332.6. Hosokawa C, Tsubakimoto M, Inoue Y, Goto T, Senju M, Yoshimura R. Radiologic features of inflammatory pseudotumor of the ureter. AJR Am J Roentgenol. 2007; 188:W202–W205.7. Gwynn ES, Clark PE. Inflammatory myofibroblastic tumor associated with renal cell carcinoma. Urology. 2005; 66:880.8. Yamamoto H, Yamaguchi H, Aishima S, Oda Y, Kohashi K, Oshiro Y, et al. Inflammatory myofibroblastic tumor versus IgG4-related sclerosing disease and inflammatory pseudotumor: a comparative clinicopathologic study. Am J Surg Pathol. 2009; 33:1330–1340.9. Deshpande V, Zen Y, Chan JK, Yi EE, Sato Y, Yoshino T, et al. Consensus statement on the pathology of IgG4-related disease. Mod Pathol. 2012; 25:1181–1192.10. Divatia M, Kim SA, Ro JY. IgG4-related sclerosing disease, an emerging entity: a review of a multi-system disease. Yonsei Med J. 2012; 53:15–34.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Unique Imaging Features in Hepatic Actinomycosis Accompanied by an IgG4-Related Inflammatory Pseudotumor: A Case Report
- Hepatic Immunoglobulin G4-related Inflammatory Pseudotumor Mimicking Hepatocellular Carcinoma
- Immunoglobulin G4-Related Inflammatory Pseudotumor Presenting as a Solitary Mass in the Stomach
- Overview of the Immunoglobulin G4-related Disease Spectrum
- A Case of Intraperitoneal Immunoglobulin G4-related Inflammatory Pseudotumor
