Association of Oversized Tracheal Tubes and Cuff Overinsufflation With Postintubation Tracheal Ruptures
- Affiliations
-
- 1Department of Otolaryngology, Intensive Care Medicine and Pain Therapy, Unfallkrankenhaus Berlin, Charite Medical School, Berlin. annekatrin.coordes@charite.de
- 2Department of Anesthesiology, Intensive Care Medicine and Pain Therapy, Unfallkrankenhaus Berlin, Charite Medical School, Berlin.
- 3Department of Otorhinolaryngology-Head and Neck Surgery, Charite - Universitatsmedizin Berlin, Campus Benjamin Franklin, Berlin, Germany.
- KMID: 2128919
- DOI: http://doi.org/10.3342/ceo.2015.8.4.409
Abstract
OBJECTIVES
Postintubation tracheal ruptures (PTR) are rare but cause severe complications. Our objective was to investigate the tracheal pattern of injury resulting from cuff inflation of the tracheal tube, to study the two main factors responsible for PTR (cuff overinsufflation and inapplicable tube sizes), and to explain the context, why small women are particularly susceptible to PTR.
METHODS
Experimental study performed on 28 fresh human laryngotracheal specimens (16 males, 12 females) within 24 hours post autopsy. Artificial ventilation was simulated by using an underwater construction and a standard tracheal tube. Tube sizes were selected according to our previously published nomogram. Tracheal lesions were detected visually and tracheal diameters measured. The influence of body size, sex difference and appropriate tube size were investigated according to patient height.
RESULTS
In all 28 cases, the typical tracheal lesion pattern was a longitudinal median rupture of the posterior trachea. Appropriate tube sizes according to body size caused PTR with significantly higher cuff pressure when compared with oversized tubes. An increased risk of PTR was found in shorter patients, when oversized tubes were used. Sex difference did not have any significant influence.
CONCLUSION
This experimental model provides information about tracheal patterns in PTR for the first time. The model confirms by experiment the observations of case series in PTR patients, and therefore emphasizes the importance of correct tube size selection according to patient height. This minimizes the risk of PTR, especially in shorter patients, who have an increased risk of PTR when oversized tubes are used.
Keyword
MeSH Terms
Figure
-
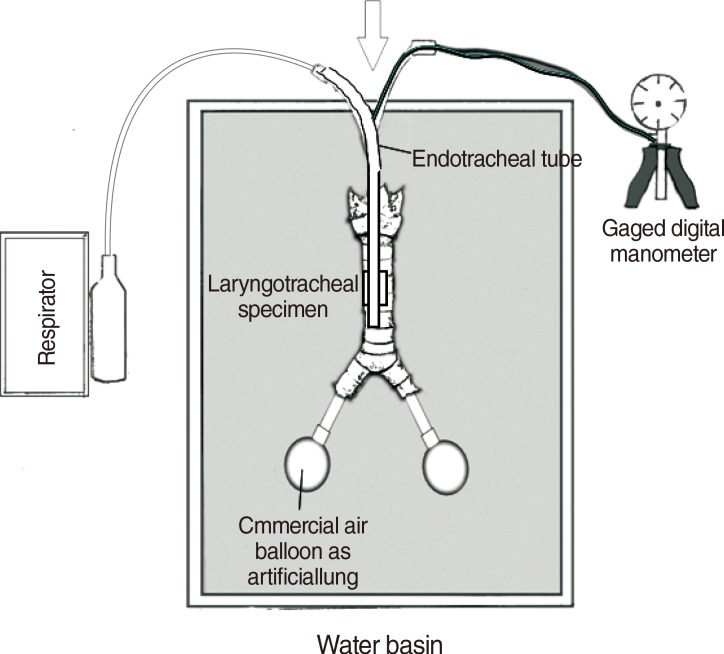
Fig. 1 Experimental setup of the artificial ventilation system. The ventilation system is connected with the trachea and main bronchi via an tracheal tube placed subglottically and with the artificial lung.
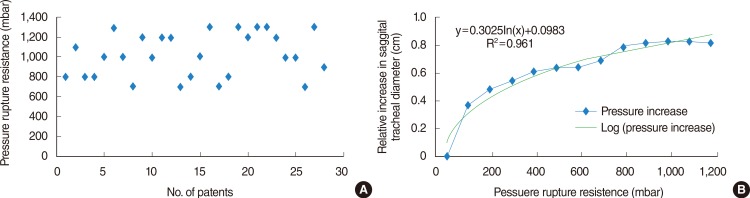
Fig. 2 Pressure rupture resistance during tracheal ruptures. (A) Pressure rupture resistance during tracheal ruptures of all investigated tracheal specimens (see Table 1) represented using a scatter diagram. (B) Relative increase in the coronal tracheal diameter with increasing pressure rupture resistance.
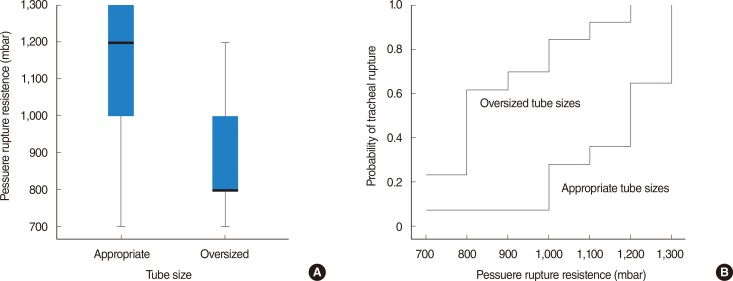
Fig. 3 Pressure rupture resistance according to suitable versus unsuitable tubes. (A) Pressure rupture resistance during tracheal ruptures of investigated tracheal specimens according to tube suitability represented using a box plot. (B) The probability of tracheal rupture is represented using the one minus probability of survival determined by Kaplan-Meier.
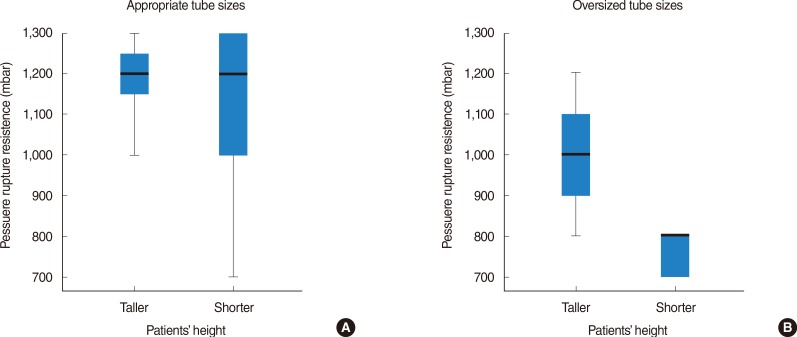
Fig. 4 Pressure rupture resistance depending on taller and shorter patients' height according to suitable (A) versus unsuitable tubes (B). Data are represented using box plots.
Reference
-
1. Minambres E, Buron J, Ballesteros MA, Llorca J, Munoz P, Gonzalez-Castro A. Tracheal rupture after endotracheal intubation: a literature systematic review. Eur J Cardiothorac Surg. 2009; 6. 35(6):1056–1062. PMID: 19369087.2. Conti M, Pougeoise M, Wurtz A, Porte H, Fourrier F, Ramon P, et al. Management of postintubation tracheobronchial ruptures. Chest. 2006; 8. 130(2):412–418. PMID: 16899839.
Article3. Cardillo G, Carbone L, Carleo F, Batzella S, Jacono RD, Lucantoni G, et al. Tracheal lacerations after endotracheal intubation: a proposed morphological classification to guide non-surgical treatment. Eur J Cardiothorac Surg. 2010; 3. 37(3):581–587. PMID: 19748275.
Article4. Chen EH, Logman ZM, Glass PS, Bilfinger TV. A case of tracheal injury after emergent endotracheal intubation: a review of the literature and causalities. Anesth Analg. 2001; 11. 93(5):1270–1271. PMID: 11682412.
Article5. Lim H, Kim JH, Kim D, Lee J, Son JS, Kim DC, et al. Tracheal rupture after endotracheal intubation: a report of three cases. Korean J Anesthesiol. 2012; 3. 62(3):277–280. PMID: 22474557.6. Wagner A, Roeggla M, Hirschl MM, Roeggla G, Schreiber W, Sterz F. Tracheal rupture after emergency intubation during cardiopulmonary resuscitation. Resuscitation. 1995; 12. 30(3):263–266. PMID: 8867716.
Article7. Schedlbauer EM, Todt I, Ernst A, Seidl RO. Iatrogenic tracheal rupture in children: a retrospective study. Laryngoscope. 2009; 3. 119(3):571–575. PMID: 19160397.
Article8. Weiss M, Dullenkopf A, Gysin C, Dillier CM, Gerber AC. Shortcomings of cuffed paediatric tracheal tubes. Br J Anaesth. 2004; 1. 92(1):78–88. PMID: 14665558.9. Randestad A, Lindholm CE, Fabian P. Dimensions of the cricoid cartilage and the trachea. Laryngoscope. 2000; 11. 110(11):1957–1961. PMID: 11081618.
Article10. Medina CR, Camargo Jde J, Felicetti JC, Machuca TN, Gomes Bde M, Melo IA. Post-intubation tracheal injury: report of three cases and literature review. J Bras Pneumol. 2009; 8. 35(8):809–813. PMID: 19750335.11. Marty-Ane CH, Picard E, Jonquet O, Mary H. Membranous tracheal rupture after endotracheal intubation. Ann Thorac Surg. 1995; 11. 60(5):1367–1371. PMID: 8526628.12. Sippel M, Putensen C, Hirner A, Wolff M. Tracheal rupture after endotracheal intubation: experience with management in 13 cases. Thorac Cardiovasc Surg. 2006; 2. 54(1):51–56. PMID: 16485190.
Article13. Seegobin RD, van Hasselt GL. Endotracheal cuff pressure and tracheal mucosal blood flow: endoscopic study of effects of four large volume cuffs. Br Med J (Clin Res Ed). 984; 3. 288(6422):965–968.
Article14. Guyton D, Banner MJ, Kirby RR. High-volume, low-pressure cuffs. Are they always low pressure. Chest. 1991; 10. 100(4):1076–1081. PMID: 1914561.15. Sengupta P, Sessler DI, Maglinger P, Wells S, Vogt A, Durrani J, et al. Endotracheal tube cuff pressure in three hospitals, and the volume required to produce an appropriate cuff pressure. BMC Anesthesiol. 2004; 11. 4(1):8. PMID: 15569386.
Article16. Hoffman RJ, Parwani V, Hahn IH. Experienced emergency medicine physicians cannot safely inflate or estimate endotracheal tube cuff pressure using standard techniques. Am J Emerg Med. 2006; 3. 24(2):139–143. PMID: 16490640.
Article17. Michlig SA. Anaesthetic staff cannot identify extremely high tracheal tube cuff pressures by palpation of the pilot balloon. Br J Anaesth. 2013; 8. 111(2):300–301. PMID: 23858076.
Article18. Li Bassi G, Ranzani OT, Marti JD, Giunta V, Luque N, Isetta V, et al. An in vitro study to assess determinant features associated with fluid sealing in the design of endotracheal tube cuffs and exerted tracheal pressures. Crit Care Med. 2013; 2. 41(2):518–526. PMID: 23263575.
Article19. Ulrich-Pur H, Hrska F, Krafft P, Friehs H, Wulkersdorfer B, Kostler WJ, et al. Comparison of mucosal pressures induced by cuffs of different airway devices. Anesthesiology. 2006; 5. 104(5):933–938. PMID: 16645443.
Article20. Horisberger T, Gerber S, Bernet V, Weiss M. Measurement of tracheal wall pressure: a comparison of three different in vitro techniques. Anaesthesia. 2008; 4. 63(4):418–422. PMID: 18336493.
Article21. Striebel HW, Pinkwart LU, Karavias T. Tracheal rupture caused by overinflation of endotracheal tube cuff. Anaesthesist. 1995; 3. 44(3):186–188. PMID: 7762778.22. Seidl RO, Todt I, Nielitz T, Ernst A. Tracheal ruptures in endotracheal intubation: diagnosis and therapy. HNO. 2002; 2. 50(2):134–138. PMID: 12080623.23. Stannard K, Wells J, Cokis C. Tracheal rupture following endotracheal intubation. Anaesth Intensive Care. 2003; 10. 31(5):588–591. PMID: 14601288.
Article24. Coordes A, Rademacher G, Knopke S, Todt I, Ernst A, Estel B, et al. Selection and placement of oral ventilation tubes based on tracheal morphometry. Laryngoscope. 2011; 6. 121(6):1225–1230. PMID: 21557233.
Article25. Dullenkopf A, Gerber AC, Weiss M. Nitrous oxide diffusion into tracheal tube cuffs: comparison of five different tracheal tube cuffs. Acta Anaesthesiol Scand. 2004; 10. 48(9):1180–1184. PMID: 15352966.
Article26. Chadha NK, Gordin A, Luginbuehl I, Patterson G, Campisi P, Taylor G, et al. Automated cuff pressure modulation: a novel device to reduce endotracheal tube injury. Arch Otolaryngol Head Neck Surg. 2011; 1. 137(1):30–34. PMID: 21242543.27. Massard G, Rouge C, Dabbagh A, Kessler R, Hentz JG, Roeslin N, et al. Tracheobronchial lacerations after intubation and tracheostomy. Ann Thorac Surg. 1996; 5. 61(5):1483–1487. PMID: 8633963.
Article28. Lampl L. Tracheobronchial injuries: conservative treatment. Interact Cardiovasc Thorac Surg. 2004; 6. 3(2):401–405. PMID: 17670273.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Airway obstruction due to post intubation circumferential tracheal web formation: A case report
- Postintubation Tracheal Ruptures: A case report
- Delayed diagnosis of postintubation tracheal laceration in a patient who underwent septorhinoplasty including osteotomy: A case report
- A Case of Postintubation Tracheal Stenosis Treated by Endoscopic Nd-YAG Laser and Balloon Catheter
- Leakage of fluid around endotracheal tube cuffs: a cadaver study
