Solitary Fibrous Tumor of Central Nervous System: A Case Report
- Affiliations
-
- 1Department of Neurosurgery, National Health Insurance Service Ilsan Hospital, Goyang, Korea. khyang@nhimc.or.kr
- 2Department of Radiology, National Health Insurance Service Ilsan Hospital, Goyang, Korea.
- 3Department of Pathology, National Health Insurance Service Ilsan Hospital, Goyang, Korea.
- KMID: 2114660
- DOI: http://doi.org/10.14791/btrt.2015.3.2.127
Abstract
- Solitary fibrous tumor (SFT) is a rare neoplasm of mesenchymal origin, especially in the central nervous system (CNS). Reported herein is a case of SFT of CNS in a 63-year-old female patient who had confused mentality, without other neurological deficit. The brain MRI showed an ovoid mass in the right frontal lobe. The tumor was surgically removed grossly and totally, and the pathologic diagnosis was SFT. At 55 months after the surgery, the tumor recurred at the primary site and at an adjacent area. A second operation was thus done, and the tumor was again surgically removed grossly and totally. The pathologic diagnosis was the same as the previous, but the Ki-67 index was elevated. Ten months later, two small recurring tumors in the right frontal skull base were found in the follow-up MRI. It was decided that radiation therapy be done, and MRI was done again 3 months later. In the follow-up MRI, the size of the recurring mass was found to have decreased, and the patient did not manifest any significant symptom. Follow-up will again be done 18 months after the second surgery.
MeSH Terms
Figure
-
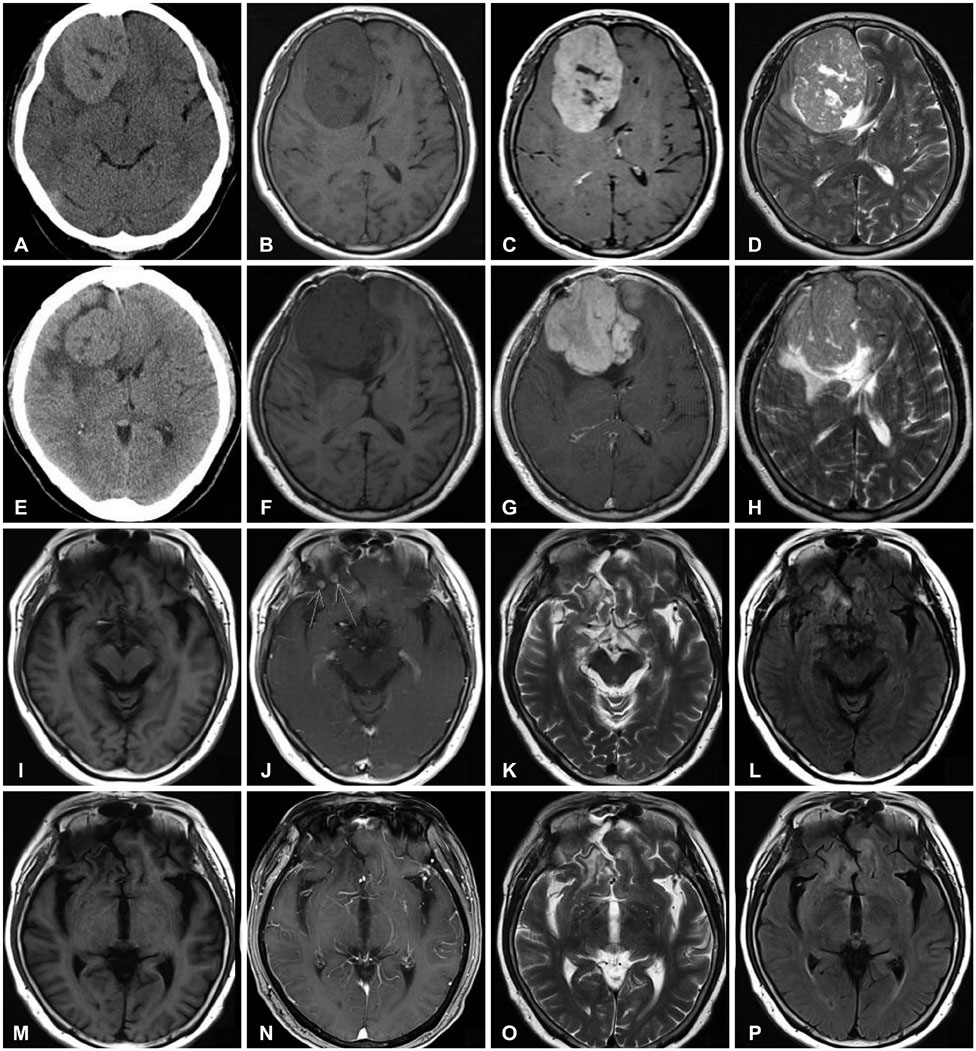
Fig. 1 Preoperative image shows about 8.0×5.2×6.4 cm3 sized ovoid mass in the right frontal convexity. A: CT shows iso to high density with parenchyma. B: T1WI shows intermediate-low signal intensity. C: T2WI shows intermediate-low signal intensity and in upper and medial portion of this mass, there are lesions with relatively low signal intensity. D: Gd-enhanced T1WI shows relatively strong enhancement. Postoperative 55 months MRI shows recurrence of tumor. E: CT shows isodensity mass with around low density with parenchyma. F: T1WI shows intermediate-low signal intensity. G: T2WI shows intermediate-high signal intensity. H: Gd-enhanced T1WI shows relatively strong enhancement. After 10 months second surgery, MRI shows a few small recurred nodule in right frontal base. I: T1WI. J: Gd-enhanced T1WI shows small nodule (arrows) in right frontal base. K: T2WI. L: FLAIR. After 3 months IMRT, MRI shows decreased size of nodule. M: T1WI. N: Gd-enhanced T1WI. O: T2WI. P: FLAIR. T1WI, T1-weighted image; T2WI, T2-weighted image; FLAIR, fluid attenuated inversion recovery; IMRT, intensity-modulated radiation therapy.
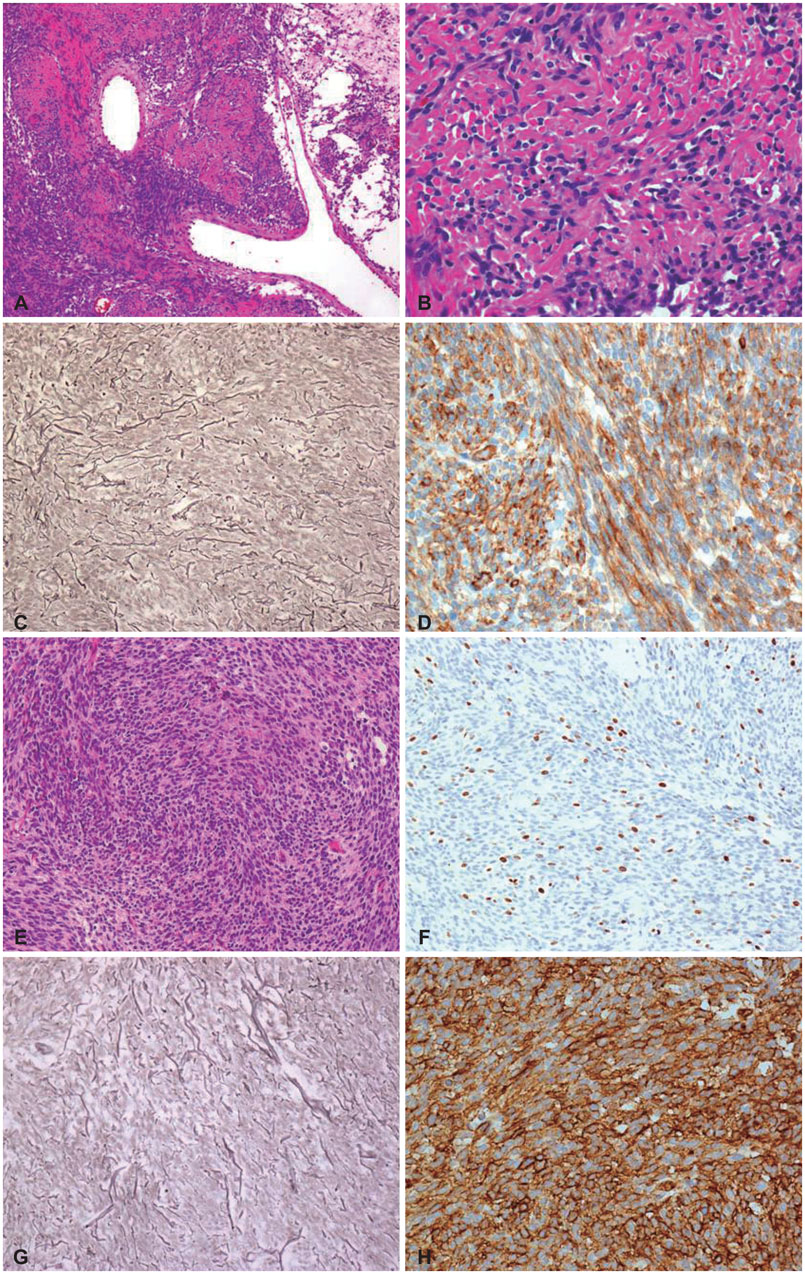
Fig. 2 Immunohistochemical features of first operation. A: On histologic examination of lower power view, mixed hypercellular and hypocellular area are seen with multifocally laid down collagen and occasional staghorn-like vessels (H&E, ×100). B: On high power field, relatively homogenous short spindle tumor cells in intervening collagens are seen (H&E, ×400). C: Sparse reticulin fibers are observed among tumor cells contrary to hemangiopericytoma (reticulin stain, ×200). D: The tumor cells show diffuse strong reactivity for CD34 on immunohistochemical stain (CD34, ×400). H&E, hematoxylin and eosin.
Reference
-
1. Musyoki FN, Nahal A, Powell TI. Solitary fibrous tumor: an update on the spectrum of extrapleural manifestations. Skeletal Radiol. 2012; 41:5–13.
Article2. Hu SW, Tsai KB, Yang SF, Lee KS, Chai CY. Unusual solitary fibrous tumors in the central nervous system: a report of two cases. Kaohsiung J Med Sci. 2005; 21:179–184.
Article3. Brunori A, Cerasoli S, Donati R, Giangaspero F, Chiappetta F. Solitary fibrous tumor of the meninges: two new cases and review of the literature. Surg Neurol. 1999; 51:636–640.
Article4. Bisceglia M, Dimitri L, Giannatempo G, et al. Solitary fibrous tumor of the central nervous system: report of an additional 5 cases with comprehensive literature review. Int J Surg Pathol. 2011; 19:476–486.
Article5. Ambrosini-Spaltro A, Eusebi V. Meningeal hemangiopericytomas and hemangiopericytoma/solitary fibrous tumors of extracranial soft tissues: a comparison. Virchows Arch. 2010; 456:343–354.
Article6. Park MS, Araujo DM. New insights into the hemangiopericytoma/solitary fibrous tumor spectrum of tumors. Curr Opin Oncol. 2009; 21:327–331.
Article7. Wang XQ, Zhou Q, Li ST, Liao CL, Zhang H, Zhang BY. Solitary fibrous tumors of the central nervous system: clinical features and imaging findings in 22 patients. J Comput Assist Tomogr. 2013; 37:658–665.8. Weon YC, Kim EY, Kim HJ, Byun HS, Park K, Kim JH. Intracranial solitary fibrous tumors: imaging findings in 6 consecutive patients. AJNR Am J Neuroradiol. 2007; 28:1466–1469.
Article9. Caroli E, Salvati M, Orlando ER, Lenzi J, Santoro A, Giangaspero F. Solitary fibrous tumors of the meninges: report of four cases and literature review. Neurosurg Rev. 2004; 27:246–251.10. Ginat DT, Bokhari A, Bhatt S, Dogra V. Imaging features of solitary fibrous tumors. AJR Am J Roentgenol. 2011; 196:487–495.
Article11. Fargen KM, Opalach KJ, Wakefield D, Jacob RP, Yachnis AT, Lister JR. The central nervous system solitary fibrous tumor: a review of clinical, imaging and pathologic findings among all reported cases from 1996 to 2010. Clin Neurol Neurosurg. 2011; 113:703–710.
Article12. Münks S. [Solitary fibrous tumor (SFT) of the nasal mucosa]. Laryngorhinootologie. 2003; 82:655–658.13. Macfarlane RG, Galloway M, Plowman PN, Thomas DG. A highly vascular intracranial solitary fibrous tumor treated with radiotherapy and toremifene: case report. Neurosurgery. 2005; 56:E1378.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Intradural Solitary Fibrous Tumor in the Thoracic Spine: A Case Report
- Myxoid Solitary Fibrous Tumor of the Central Nervous System
- Is a Solitary Fibrous Tumor in the External Auditory Canal Benign?
- Solitary Fibrous Tumor of the Adrenal Gland: A Case Report
- Case of a Metastatic Solitary Fibrous Tumor Presenting as Gastrointestinal Bleeding
