J Korean Soc Endocrinol.
2005 Aug;20(4):390-394. 10.3803/jkes.2005.20.4.390.
A Case of Bilateral Macronodular Adrenocortical Hyperplasia Accompanied by Hyperresponsiveness to Vasopressin
- Affiliations
-
- 1Department of Internal Medicine, Inha University, College of Medicine, Incheon, Korea, Department of Surgery, Korea.
- KMID: 2100471
- DOI: http://doi.org/10.3803/jkes.2005.20.4.390
Abstract
- Cushing's syndrome associated with nodular adrenal hyperplasia glands is divided into 4 main categories: adrenal adenoma, adrenal carcinoma, primary pigmented nodular adrenal dysplasia and macronodular adrenal hyperplasia(MAH). The mechanism of bilateral MAH, when ACTH is suppressed, was previously unknown, and referred to as being "autonomous". Recently, several reports have shown MAH to be under the control of ectopic or eutopic membrane hormone. Here, a case of Cushing's syndrome, caused by bilateral MAH, is reported. A 62-year-old woman presented with Cushingoid features, hypertension and diabetes mellitus. In her case, abnormal adrenal stimulation of cortisol secretion in response to exogenous vasopression stimulation was shown. Her urine free cortisol was 726.0microgram/dL, which was not suppressed after administration of high-dose dexamethasone. Her plasma cortisol level was elevated, but without circadian rhythm. ACTH was undetectable. An abdomen CT scan demonstrated bilaterally enlarged multinodular adrenal glands. A Sella MRI revealed no alteration of the pituitary gland. The patient underwent a laparoscopic bilateral adrenalectomy. Histological examination revealed bilateral macronodular hyperplasia. After having recovered, the patient showed progressive regression of the Cushingoid status.
MeSH Terms
-
Abdomen
Adenoma
Adrenal Glands
Adrenalectomy
Adrenocorticotropic Hormone
Circadian Rhythm
Cushing Syndrome
Dexamethasone
Diabetes Mellitus
Female
Humans
Hydrocortisone
Hyperplasia*
Hypertension
Magnetic Resonance Imaging
Membranes
Middle Aged
Pituitary Gland
Plasma
Tomography, X-Ray Computed
Vasopressins*
Adrenocorticotropic Hormone
Dexamethasone
Hydrocortisone
Vasopressins
Figure
-
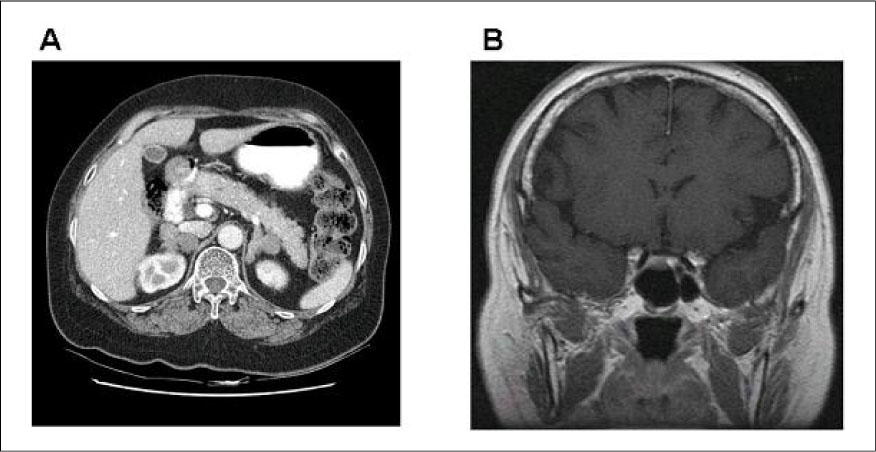
Fig. 1 A) abdominal CT (with contrast) shows bilaterally enlarged multinodular adrenal glands. B) Brain MRI (T1 with Gd enhancement) shows no abnormalities of pituitary gland.

Fig. 2 A) & B) Gross appearance shows multinodular yellowish brown soft tissue. C) & D) Microscopic view (×10, C) (×200, D) revealed macronodular hyperplasia.
Reference
-
1. Orth DN. The old and the new in Cushing's syndrome. N Eng J Med. 1984. 310:649–654.2. Aron DC, Findling JW, Brooks RM, Fisher FE, Forsham PH, Tyrrell JB. Pituitary ACTH dependency of nodular adrenal hyperplasia in Cushing's syndrome; Report of two cases and review of the literature. Am J Med. 1981. 71:302–306.3. Samuels MH, Loriaux DL. Cushing's syndrome and nodular adrenal gland. Endocrinol Metab Clin North Am. 1994. 23:555–569.4. Fukata J, Nakai Y, Imura H, Abe K, Aono T, Demura H, Fujita T, Hibi I, Ibayashi H, Igarashi M. Human corticotropin-releasing hormone test in normal subjects and patients with hypothalamic pitiutary or adrenocortical disorders. Endocr J. 1988. 35:491–501.5. Shenoy BV, Carpenter PC, Carney JA. Bilateral primary pigmented nodular adrenocortical disease. Am J Surg Pathol. 1984. 8:335–344.6. Irie J, Kawai K, Shigematsum K, Suzuji S, Nomata K, Minami Y, Kanetake H. Adrenocorticotropic hormone-independent bilateral macronodular adrenocortical hyperplasia associated with Cushing's syndrome. Pathol Int. 1995. 45:240–246.8. Lacroix A, Bolte E, Tremblay J, Dupre J, Poitras P, Fournier H, Garon J, Garrel D, Bayard F, Taillefer R, Flanagan RJ, Hamet P. Gastric inhibitory polypeptide-dependent cortisol hypersecretion-a new cause of Cushing's syndrome. N Engl J Med. 1992. 327:974–980.9. Yanovski JA, Cutler GB Jr. Glucocorticoid action and the clinical features of Cushing's syndrome. Endocrinol Metab Clin North Am. 1994. 23:487–509.10. Newell-Price J, Trainer P, Besser M, Grossman A. The diagnosis and differential diagnosis of Cushing's syndrome and pseudo-Cushing's states. Endocr Rev. 1998. 19:647–672.11. Trainer PJ, Grossman A. The diagnosis and differential diagnosis of Cushing's syndrome. Clin Endocrinol. 1991. 34:317–330.12. Joffe SN, Brown C. Nodular adrenal hyperplasia and Cushing's syndrome. Surgery. 1983. 94:919–925.13. Iida S, Nakamura Y, Fujii H, Nishimura J, Tsugawa M, Gomi M, Fukata J, Tarui S, Moriwaki K, Kitani T. A patient with hypocortisolism and Cushing's syndrome-like manifestations: cortisol hyperreactive syndrome. J Clin Endocrinol Metab. 1990. 79:729–737.14. Sasano H, Miyazaki S, Sawai T, Sasano N, Nagura H, Funahashi H, Aiba M, Demura H. Primary pigmented nodular adrenocortical disease (PPNAD): immunohistochemical and in situ hybridization analysis of steroidogenic enzymes in eight cases. Endocr Pathol. 1992. 3:23–29.15. Schorr I, Ney RL. Abnormal hormone responses of an adrenocortical cancer adenyl cyclase. J Clin Invest. 1971. 50:1295–1300.16. Lacroix A, Ndiaye N, Tremblay J, Hamet P. Ectopic and abnormal hormone receptors in adrenal Cushing's syndrome. Endocr Rev. 2001. 22:75–110.17. Lacroix A, Tremblay J, Rousseau G, Bouvier M, Hamet P. Propranolol therapy for ectopic beta-adrenergic receptors in adrenal Cushing's syndrome. N Eng J Med. 1997. 337:1429–1434.18. Seron-Ferre M, Lawrence CC, Jaffe RB. Role of hCG in regulation of the fetal zone of the human fetal adrenal gland. J Clin Endocrinol Metab. 1978. 46:834–837.19. Mune T, Murase H, Yamakita N, Fukuda T, Murayama M, Miura A, Suwa T, Hanafusa J, Daido H, Morita H, Yasuda K. Eutopic overexpression of vasopressin v1a receptor in adrenocorticotropin-independent macronodular adrenal hyperplasia. J Clin Endocrinol Metab. 2002. 87:5706–5713.20. Lefebvre H, Gonzalez KN, Contesse V, Delarue C, Vaudry H, Kuhnl JM. Effect of prolonged administration of the serotonin4 (5-HT4) receptor agonist cisapride on aldosterone secretion in healthy volunteers. Endocr Res. 1998. 24:749–752.21. Horiba N, Suda T, Aiba M, Naruse M, Nomura K, Imamura M, Demura H. Lysine vasopressin stimulation of cortisol secretion in patients with adrenocorticotropin-independent macronodular adrenal hyperplasia. J Clin Endocrinol Metab. 1995. 80:2336–2341.22. Mircescu H, Jilwan J, N'Diaye N, Bourdeau I, Tremblay J, Hamet P, Lacroix A. Are ectopic or abnormal membrane hormone receptors frequently present in adrenal Cushing's syndrome? J Clin Endocrinol Metab. 2000. 85:3531–3536.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Bilateral Macronodular Adrenocortical Hyperplasia
- A Case of AVP Dependent Bilateral Macronodular Adrenal Hyperplasia
- Adrenocorticotropic hormone-independent macronodular adrenal hyperplasia with abnormal cortisol secretion mediated by catecholamines
- Cushing Syndrome Caused by ACTH-independent Macronodular Adrenal Hyperplasia
- A case of macronodular adrenocortical hyperplasia
