J Korean Soc Radiol.
2011 Feb;64(2):109-112. 10.3348/jksr.2011.64.2.109.
Acute Cerebral Infarction after FK 506 Administration in a Kidney Transplantation Recipient: A Case Report
- Affiliations
-
- 1Department of Diagnostic Radiology, College of Medicine, Yeungnam University, Daegu, Korea. wmbyun@med.yu.ac.kr
- KMID: 2097924
- DOI: http://doi.org/10.3348/jksr.2011.64.2.109
Abstract
- FK506 is widely used as a potent immunosuppressive agent following organ transplantation. However, the use of FK506 is associated with a wide spectrum of neurotoxicity. FK506-induced cerebral infarctions have rarely been reported. We report here on a case of the acute cerebral infarction caused by vasospasm after FK506 administration in a kidney transplantation recipient. There were areas with increased signal intensity on the diffusion-weighted image. The areas showing increased signal intensity on the diffusion- and T2-weighted images demonstrated decreased signal intensity on the apparent diffusion coefficient mapping. MR angiography showed diffuse stenosis in both the anterior and middle cerebral arteries.
MeSH Terms
Figure
-
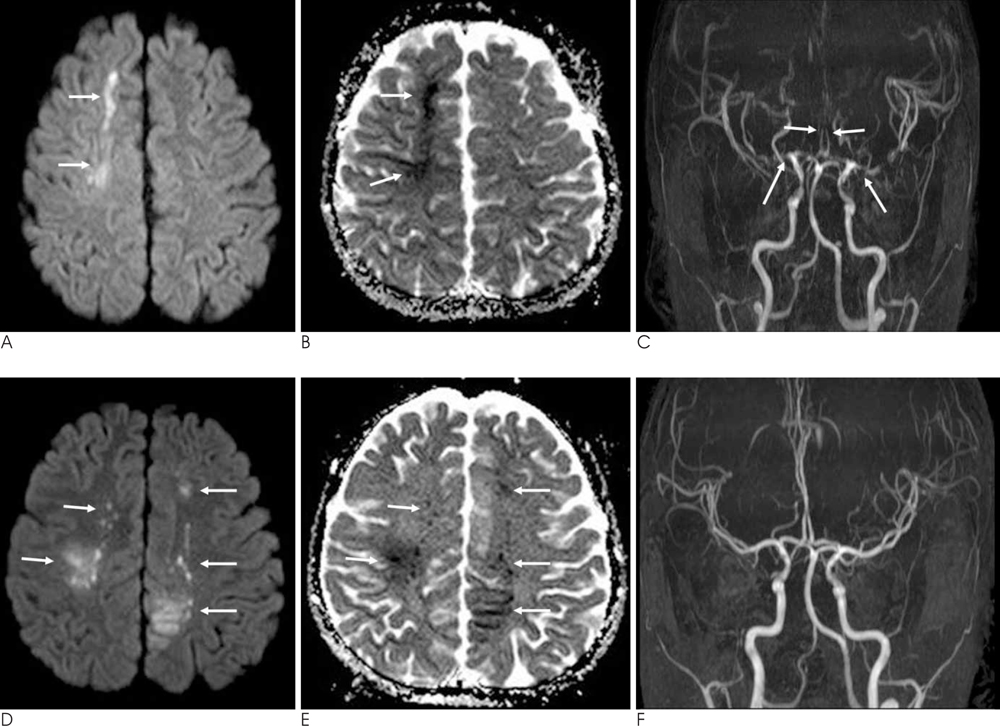
Fig. 1 Acute infarction with vasospasm caused by FK506 administration. A, B. Increased signal intensity on DWI (A) and decreased signal intensity on ADC mapping (B) in the right frontal lobe are demonstrated (arrows). The findings indicate acute infarction. C. MRA shows diffuse stenosis in both the anterior and middle cerebral arteries (arrows). D, E. Follow-up DWI (D) and ADC mapping (E) after one weak reveal another new acute infarction in both the fronto-parietal lobes (arrows). F. Improvement of vasospasm is seen on the follow-up MRA one month after the discontinuation of FK506.
Reference
-
1. Gijtenbeek JM, van den Bent MJ, Vecht CJ. Cyclosporine neurotoxicity: a review. J Neurol. 1999; 246:339–346.2. Basic-Jukic N, Basic-Kes V, Kes P, Furic-Cunko V, Bacic-Baronica K. Neurological complications in renal transplant recipients. Acta Med Croatica. 2008; 62:Suppl 1. 76–81.3. Ahn KJ, Lee JW, Hahn ST, Yang DW, Kim PS, Kim HJ, et al. Diffusion-weighted MRI and ADC mapping in FK506 neurotoxicity. Br J Radiol. 2003; 76:916–919.4. Kinoshita T, Moritani T, Shrier DA, Hiwatashi A, Wang HZ, Numaguchi Y, et al. Diffusion-weighted MR imaging of posterior reversible leukoencephalopathy syndrome: a pictorial essay. Clin Imaging. 2003; 27:307–315.5. Keenan RJ, Konishi H, Kawai A, Paradis IL, Nunley DR, Iacono AT, et al. Clinical trial of tacrolimus versus cyclosporine in lung transplantation. Ann Thorac Surg. 1995; 60:580–584.6. Eidelman BH, Abu-Elmagd K, Wilson J, Fung JJ, Alessiani M, Jain A, et al. Neurologic complications of FK 506. Transplant Proc. 1991; 23:3175–3178.7. Junna MR, Rabinstein AA. Tacrolimus induced leukoencephalopathy presenting with status epilepticus and prolonged coma. J Neurol Neurosurg Psychiatry. 2007; 78:1410–1411.8. Kilinc M, Benli S, Can U, Yilmaz A, Karakayali H, Colak T, et al. FK 506-induced fulminant leukoencephalopathy after kidney transplantation: case report. Transplant Proc. 2002; 34:1182–1184.9. Curro G, Baccarani U, Adani GL, Lorenzin D, Bresadola F. Transient ischemic attack after rizatriptan administration in a liver transplant recipient: a case report. Transplant Proc. 2006; 38:3138–3139.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Effect of FK 506 on the cornea: use of topical FK 506 in corneal transplantation in a guinea pig-rat model
- A Novel Approach to Peripheral Nerve Regeneration: Local FK-506 Delivery Using a Reservoir Flap Model
- The Effect of Combined Immunosuppressive Treatment with FK 506-Cyclophosphamide on Surgical Angiogenesis
- Clinical manifestations of delayed COVID-19 pneumonia in kidney transplant recipients
- The Effects of Cyclosporin A and FK-506 on the Cytokine Production of Lymphocytes in Atopic Dermatitis
