The Subarticular Screw: a New Trajectory for the C2 Screw
- Affiliations
-
- 1Department of Orthopaedic Surgery, Seoul National University College of Medicine, Seoul, Korea. seiswon@naver.com
- 2Department of Orthopaedic Surgery, Wonkwang University School of Medicine, Iksan, Korea.
- KMID: 2097821
- DOI: http://doi.org/10.4184/jkss.2006.13.2.75
Abstract
-
STUDY DESIGN: Surgical simulation using CT images and computer software.
OBJECTIVES
We wanted to determine a new trajectory for the C2 screw, and then we wanted to evaluate its safety and accuracy. Summary of Literature REVIEW: There have been a few suggestions for trajectories of the C2 pedicle screws. However, their safety is somewhat unsatisfactory as all of them have some possibility of vertebral artery injury.
MATERIALS AND METHODS
Using 1 mm-sliced CT scan images of 158 patients and an A-view spine surgery simulator 1.0, we determined a new trajectory for the C2 screw with which 4.0 mm screws can be inserted with a minimal number of breaches of the bone cortices. The percentage of cortical perforations by the suggested trajectory was compared with that by the pedicle screws by means of simulation.
RESULTS
The medial angulation of the determined trajectory is the same as that of the pedicle on the axial CT images: it usually is between 30 and 40 degrees. The screw is angled toward the antero-superior end of the superior articular process of C2, as observed on lateral fluoroscopy. The entry point is 3 mm inferior to the posterior aspect of the superior articular surface, and this point should allows the screw (ED note: check this and it wasn't clear.)the screw to be inserted close to the superomedial border of the superior articular process. Using this trajectory, 2.5% (8/316) of the screws breached the vertebral grooves, while 6.0% (19/316) of the pedicle screws breached them (p=0.030, chi-square test).
CONCLUSIONS
The subarticular screw has improved safety compared with the pedicle screws. However, there are still some casesin which screws can not be inserted without breaching the vertebral groove. Therefore, preoperative thin-slice CT scanning with three-dimensional reconstruction and/or three-dimensional CT-angiography is recommended.
Figure
-

Fig. 1. The trajectory of the C2 subarticular screw is shown. (A) The trajectory is shown in traditional multi-planar recon-struction (MPR) images and a three-dimensional image. (B) The trajectory is shown in trajectory MPR images and a three-dimensional image. (C) A simulated lateral fluoro-scopic image shows the C2 subarticular screw trajectories.
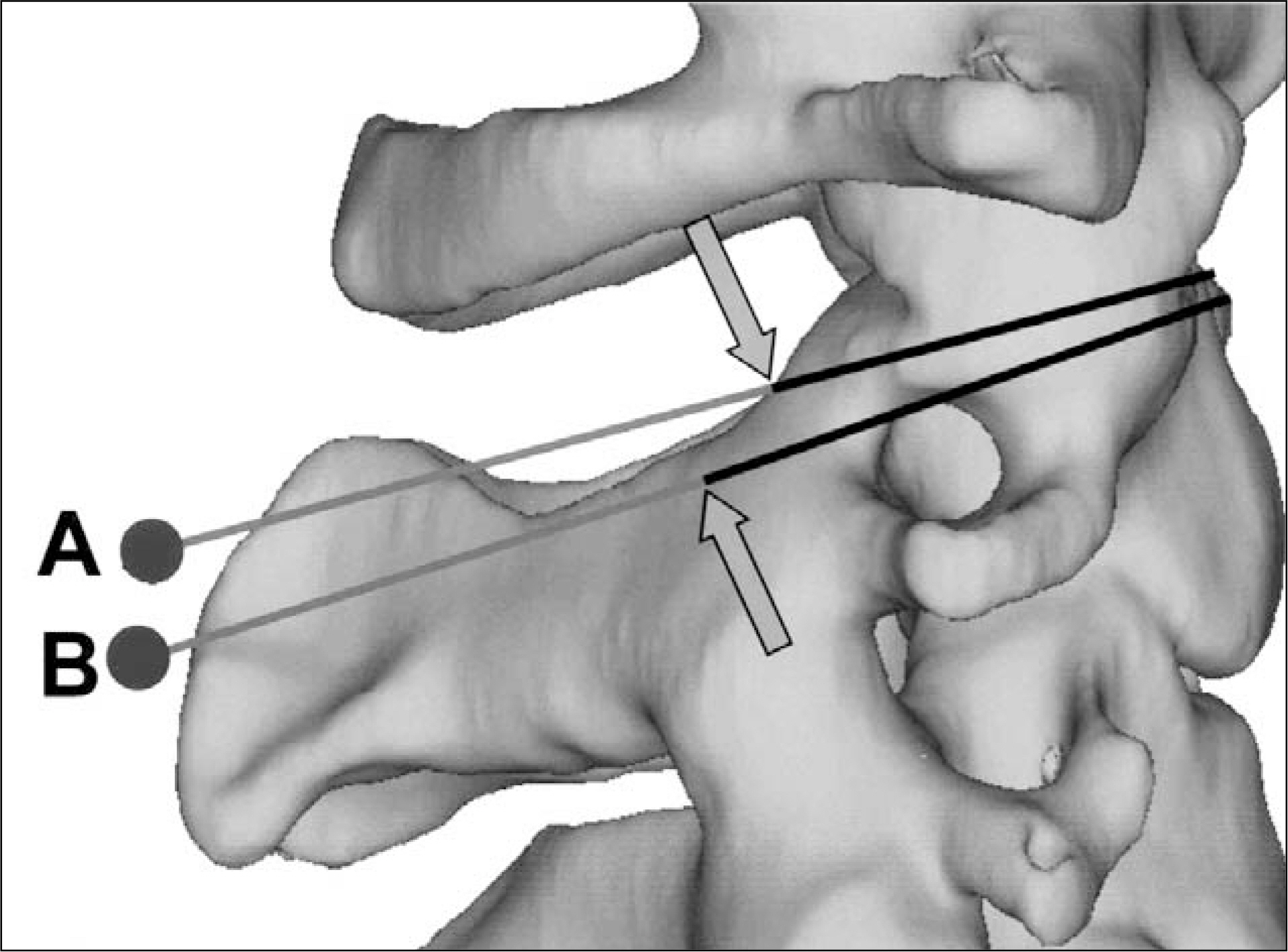
Fig. 2. Trajectories of the C2 subarticular screw (marked as "A") and the C2 pedicle screw (marked as "B") are shown. The arrows indicate the entry points of the screws. Because the entry point of the subarticular screw is superior to the pedicle screw, cortical breach at the vertebral artery groove can be frequently avoided with the former in cases in which the breach is inevitable with the latter.

Fig. 3. A case of C1-2 fixation using C1 lateral mass screws and C2 subarticular screws is shown. (A) Dynamic radiographs of a 45-year-old male show C1-2 instability. (B) The inferior view of C2 shows that the left pedicle (arrow) is too narrow for the pedicle screw. (C) An intra-operative photograph taken after polyaxial screw insertion is shown. (D) Radiographs taken 5 weeks after the operation are shown.
Cited by 3 articles
-
Indirect Decompression using Segmental Screw Fixation for Cervical Myelopathy Caused by C1-2 Subluxation - Technical Note -
Yoon Jong Kim, Kyeong Hwan Kim, Jong Hwa Won, Hak Jin Min, Ui Seong Yoon, Jin Sup Yeom
J Korean Orthop Assoc. 2007;42(6):815-821. doi: 10.4055/jkoa.2007.42.6.815.Risk of Vertebral Artery Injury: A Comparison between C2 Subarticular Segmental and C1-2 Transarticular Screws
Seong Wan Kim, Jin S. Yeom, Yoon Ju Kwon, Seung Min You, Young Hee An, Kun-Woo Park, Bong-Soon Chang, Choon-Ki Lee
J Korean Orthop Assoc. 2008;43(5):572-578. doi: 10.4055/jkoa.2008.43.5.572.Revision of Atlantoaxial Fusion using Segmental Screw Fixation: Experience in Bilateral Posterior Arch Fracture of the Atlas Complicating Atlantoaxial Halifax Clamp Fixation
Jae-Sung Suh, Kyeong-Hwan Kim, Soon-Woo Hong, Jin Sup Yeom, Kun-Woo Park, Bong-Soon Chang, Choon-Ki Lee
J Korean Soc Spine Surg. 2007;14(3):187-191. doi: 10.4184/jkss.2007.14.3.187.
Reference
-
01). Abumi K., Kaneda K. Pedicle screw fixation for nontrau-matic lesions of the cervical spine. Spine. 1997. 22:1853–1863.
Article02). Ebraheim N., Rollins JR Jr., Xu R., Jackson WT. Anatomic consideration of C2 pedicle screw placement. Spine. 1996. 21:691–695.
Article03). Goel A., Desai KI., Muzumdar DP. Atlantoaxial fixation using plate and screw method: A report of 160 treated patients. Neurosurgery. 2002. 51:1351–1356.
Article04). Harms J., Melcher RP. Posterior C1-C2 fusion with polyaxial screw and rod fixation. Spine. 2001. 26:2467–2471.
Article05). Xu R., Ebraheim NA., Missoon JR., Yeasting RA. The reliability of the lateral radiograph in determination of the optimal transarticular C1-C2 screw length. Spine. 1998. 23:2190–2194.
Article06). Xu R., Nadaud MC., Ebraheim NA., Yeasting RA. Mor-phology of the Second cervical vertebra and the posterior projection or the C2 pedicle axis. Spine. 1995. 20:259–263.07). Lee D., Yeom JS., Kwon YJ, et al. Optimal trajectories of C1 lateral mass screws and C2 pars-pedicle screws. J Kor Spine Surg. 2004. 11:202–209.08). Resnick DK., Lapsiwala S., Trost GR. Anatomic suitability of the C1-C2 complex for pedicle screw fixation. Spine. 2002. 27:1494–1498.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Atlantoaxial Fixation using C2 Subarticular Screws and C1 Lateral Mass Screws : A Technical Report
- Modified Trajectory of C2 Laminar Screw - Double Bicortical Purchase of the Inferiorly Crossing Screw
- Risk of Vertebral Artery Injury: A Comparison between C2 Subarticular Segmental and C1-2 Transarticular Screws
- Posterior Atlantoaxial Fixation with a Combination of Pedicle Screws and a Laminar Screw in the Axis for a Unilateral High-riding Vertebral Artery
- Anatomical Suitability of Posterior C1/2 Transarticular Screw Fixation in Korean
