J Korean Surg Soc.
2010 Dec;79(6):447-454. 10.4174/jkss.2010.79.6.447.
Clinical Comparative Evaluation of Open Method and Gasless or Gas Insufflation Anterior Chest Approach in Endoscopic Thyroidectomy in a Single Institution
- Affiliations
-
- 1Department of Surgery, The Catholic University of Korea College of Medicine, Uijeongbu, Korea. drbreast@catholic.ac.kr
- KMID: 2096600
- DOI: http://doi.org/10.4174/jkss.2010.79.6.447
Abstract
- PURPOSE
After the first endoscopic thyroidectomy by Huscher in 1997, several surgeons reported their experiences with endoscopic thyroidectomies. And these papers showed that clinical outcomes of endoscopic thyroidectomy are similar to conventional thyroidectomy. But, there was no randomized prospective trial to determine which approach of endoscopic thyroidectomy achieved better results. We evaluated clinical data of gasless and gas insufflation endoscopic thyroidectomies with conventional thyroidectomy to define its advantages or disadvantages.
METHODS
Between 1999 and 2009, 1,117 patients underwent thyroidectomies (1,149 cases). 747 cases was performed by conventional open method, 402 cases by endoscopic thyroidectomy. Among them, 317 cases were operated by gasless techniques and 85 cases by carbon dioxide gas insufflation.
RESULTS
Between conventional and endoscopic thyroidectomy groups, operation time, hospitalization period, tumor size, and number of retrieved lymph nodes were similar (P-value >0.05). Among 441 thyroid cancer patients, 19 had recurrence, of which 15/301 (4.98%) had conventional thyroidectomy, and 4/140 (2.85%) had endoscopic thyroidectomy. After postoperative radioactive iodine therapy, follow-up Tg levels were checked in 274 patients, the levels were <2.0 ng/ml in 87.63% (163/186) of patients after conventional thyroidectomies and in 93.18% (82/88) following endoscopic thyroidectomies. There were no significant differences (P-value=0.58). Complication incidences (hypocalcemia, hoarseness, bleeding, wound infection) in both groups were not significantly distinctive (P-value=0.58).
CONCLUSION
Minimally invasive techniques are generally applied even for malignancy in selected cases because of its advantages, such as cosmetic results. Through this study, we showed similar clinical outcomes of conventional and gasless or gas insufflations endoscopic thyroidectomy.
MeSH Terms
Figure
-
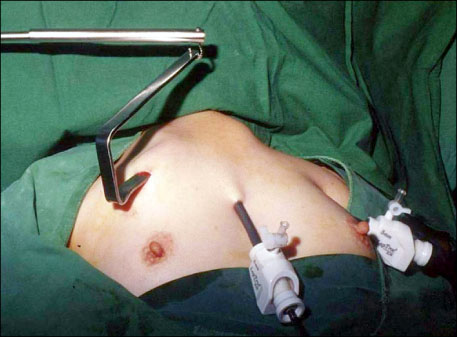
Fig. 1 Gasless endoscopic thyroidectomy. Two ports and one retractor are ready for gasless endoscopic thyroidectomy, and one axilla port is added on this setting, if needed.

Fig. 2 Four ports in gas insufflation endoscopic thyroidectomy. Endoscopic instruments access through 4 ports in axilla, areola, parasternum and midclavicular line.
Cited by 1 articles
-
Preliminary Study on Safety of Robotic or Endoscopic Thyroidectomy via Bilateral Axillo-breast Approach (BABA) without Drainage Procedure: Multicenter Trial
So Hyang Moon, Young San Jeon, Wan Wook Kim, Su Hwan Kang, Young Ju Jeong, Jung Eun Choi, Jihyoung Cho
Korean J Endocr Surg. 2015;15(2):47-51. doi: 10.16956/kaes.2015.15.2.47.
Reference
-
1. Hüscher CS, Chiodini S, Napolitano C, Recher A. Endoscopic right thyroid lobectomy. Surg Endosc. 1997. 11:877.2. Ikeda Y, Takami H, Sasaki Y, Takayama J, Niimi M, Kan S. Clinical benefits in endoscopic thyroidectomy by the axillary approach. J Am Coll Surg. 2003. 196:189–195.3. Park CS, Chung WY, Chang HS. Minimally invasive open thyroidectomy. Surg Today. 2001. 31:665–669.4. Takami H, Ikeda Y. Total endoscopic thyroidectomy. Asian J Surg. 2003. 26:82–85.5. Ikeda Y, Takami H, Tajima G, Sasaki Y, Takayama J, Kurihara H, et al. Total endoscopic thyroidectomy: axillary or anterior chest approach. Biomed Pharmacother. 2002. 56:Suppl 1. 72s–78s.6. Ohgami M, Ishii S, Arisawa Y, Ohmori T, Noga K, Furukawa T, et al. Scarless endoscopic thyroidectomy: breast approach for better cosmesis. Surg Laparosc Endosc Percutan Tech. 2000. 10:1–4.7. Shimizu K, Akira S, Jasmi AY, Kitamura Y, Kitagawa W, Akasu H, et al. Video-assisted neck surgery: endoscopic resection of thyroid tumors with a very minimal neck wound. J Am Coll Surg. 1999. 188:697–703.8. Shimizu K, Tanaka S. Asian perspective on endoscopic thyroidectomy -- a review of 193 cases. Asian J Surg. 2003. 26:92–100.9. Yamashita H, Watanabe S, Koga Y, Masatsugu T, Uchino S, Noguchi S. Total endoscopic and video-assisted thyroidectomy: cervical approach. Biomed Pharmacother. 2002. 56:Suppl 1. 64s–67s.10. Bellantone R, Lombardi CP, Rubino F, Perilli V, Sollazzi L, Mastroianni G, et al. Arterial PCO2 and cardiovascular function during endoscopic neck surgery with carbon dioxide insufflation. Arch Surg. 2001. 136:822–827.11. Gagner M. Endoscopic subtotal parathyroidectomy in patients with primary hyperparathyroidism. Br J Surg. 1996. 83:875.12. Yeung GH. Endoscopic surgery of the neck: a new frontier. Surg Laparosc Endosc. 1998. 8:227–232.13. Ochiai R, Takeda J, Noguchi J, Ohgami M, Ishii S. Subcutaneous carbon dioxide insufflation does not cause hypercarbia during endoscopic thyroidectomy. Anesth Analg. 2000. 90:760–762.14. Yeh TS, Jan YY, Hsu BR, Chen KW, Chen MF. Video-assisted endoscopic thyroidectomy. Am J Surg. 2000. 180:82–85.15. Inabnet WB 3rd, Jacob BP, Gagner M. Minimally invasive endoscopic thyroidectomy by a cervical approach. Surg Endosc. 2003. 17:1808–1811.16. Park YL, Han WK, Bae WG. 100 cases of endoscopic thyroidectomy: breast approach. Surg Laparosc Endosc Percutan Tech. 2003. 13:20–25.17. Lombardi CP, Raffaelli M, de Crea C, Princi P, Castaldi P, Spaventa A, et al. Report on 8 years of experience with video-assisted thyroidectomy for papillary thyroid carcinoma. Surgery. 2007. 142:944–951.18. Jeong JJ, Kang SW, Yun JS, Sung TY, Lee SC, Lee YS, et al. Comparative study of endoscopic thyroidectomy versus conventional open thyroidectomy in papillary thyroid microcarcinoma (PTMC) patients. J Surg Oncol. 2009. 100:477–480.19. Bergamaschi R, Becouarn G, Ronceray J, Arnaud JP. Morbidity of thyroid surgery. Am J Surg. 1998. 176:71–75.20. de Roy van Zuidewijn DB, Songun I, Kievit J, van de Velde CJ. Complications of thyroid surgery. Ann Surg Oncol. 1995. 2:56–60.21. Kitano H, Fujimura M, Kinoshita T, Kataoka H, Hirano M, Kitajima K. Endoscopic thyroid resection using cutaneous elevation in lieu of insufflation. Surg Endosc. 2002. 16:88–91.22. Kebebew E, Clark OH. Differentiated thyroid cancer: "complete" rational approach. World J Surg. 2000. 24:942–951.23. Miccoli P, Elisei R, Materazzi G, Capezzone M, Galleri D, Pacini F, et al. Minimally invasive video-assisted thyroidectomy for papillary carcinoma: a prospective study of its completeness. Surgery. 2002. 132:1070–1073. discussion 3-4.24. Bellantone R, Lombardi CP, Raffaelli M, Alesina PF, De Crea C, Traini E, et al. Video-assisted thyroidectomy for papillary thyroid carcinoma. Surg Endosc. 2003. 17:1604–1608.25. Lombardi CP, Raffaelli M, Princi P, Lulli P, Rossi ED, Fadda G, et al. Safety of video-assisted thyroidectomy versus conventional surgery. Head Neck. 2005. 27:58–64.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparative Study of Unilateral Axillo-Breast Approach with Gas Insufflation Versus Gasless Transaxillary Approach for Endoscopic Thyroidectomy in a Single Institute
- Nationwide Multicenter Survey for Current Status of Endoscopic Thyroidectomy in Korea
- A Clinical Analysis of Endoscopic Thyroidectomy by the Axillary and Anterior Chest Approach
- Gasless Endoscopic Thyroidectomy
- Gasless Endoscopic Thyroidectomy Via an Axillary Approach: Experience of 30 Cases
