Nationwide Multicenter Survey for Current Status of Endoscopic Thyroidectomy in Korea
- Affiliations
-
- 1Department of Otolaryngology-Head and Neck Surgery, Soonchunhyang University Bucheon Hospital, Soonchunhyang University College of Medicine, Bucheon, Korea. lsw0922@schmc.ac.kr
- KMID: 2360786
- DOI: http://doi.org/10.3342/ceo.2015.8.2.149
Abstract
OBJECTIVES
We evaluated the current status of endoscopic thyroidectomy procedures in Korea in terms of indications, contraindications, advantages, disadvantages, complications, and limitations of each approach.
METHODS
An email survey, consisting of 15 questions, was sent to 29 experienced endoscopic thyroidectomy surgeons.
RESULTS
The most commonly used approach was the gasless transaxillary approach (66.7%), followed by the bilateral axillo-breast approach with gas insufflation (23.8%). The most common indication was less than 1 cm, single papillary thyroid cancer. The role of endoscopic thyroidectomy is not still established; some consider it a novel procedure (34.8%), others a transition to robotic thyroidectomy (34.8%).
CONCLUSION
Our results shed light on the general consensus of opinions about endoscopic thyroidectomy, such as the advantages, disadvantages, complications, limitations, and even its future role.
Keyword
MeSH Terms
Figure
-
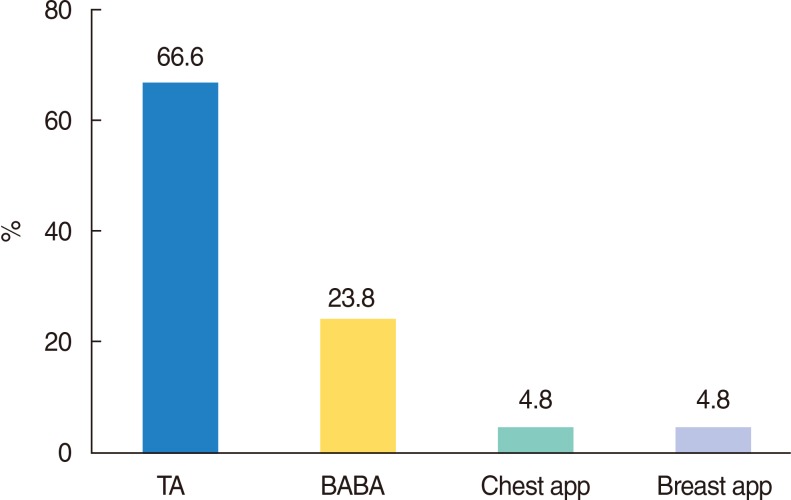
Fig. 1 Currently used approaches for endoscopic thyroidectomy. TA, gaseless transaxillary approach; BABA, bilateral axillo-breast approach with gas insufflation; Chest app, chest approach with gas insufflation; Breast app, breast approach with gas insufflation.
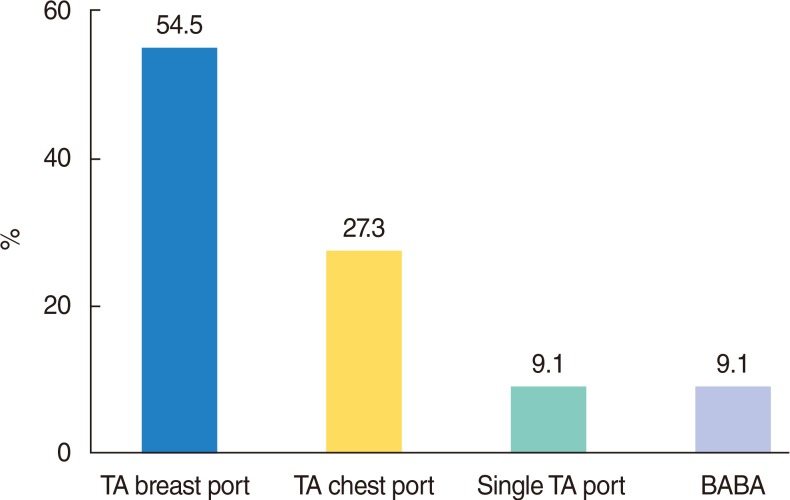
Fig. 2 Currently used approaches for endoscopic thyroidectomy by head and neck surgeons. TA breast port, transaxillary approach with breast port; TA chest port, transaxillary approach with chest port; Single TA port, single port transaxillary approach; BABA, bilateral axillo-breast approach with gas insufflation.
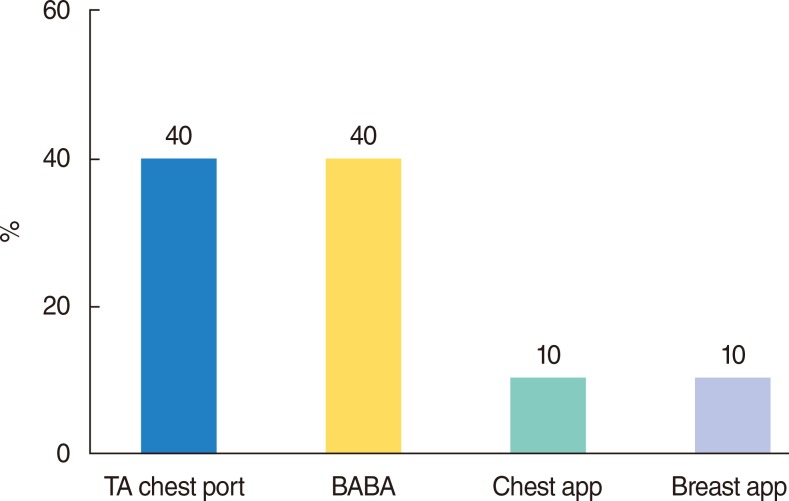
Fig. 3 Currently used approaches for endoscopic thyroidectomy by endocrine surgeons. TA, gaseless transaxillary approach; BABA, bilateral axillo-breast approach with gas insufflation; Chest app, chest approach with gas insufflation; Breast app, breast approach with gas insufflation.
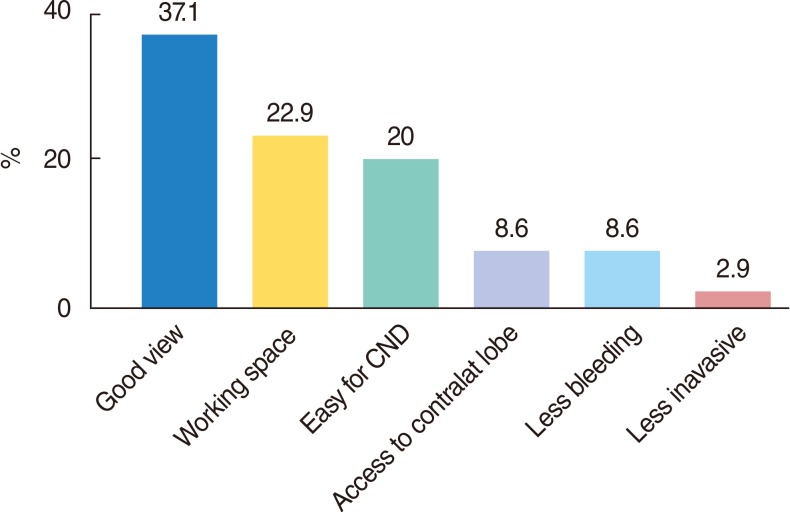
Fig. 4 Advantages of the transaxillary approach. Good view, good surgical view; Working space, enough working space; CND, central compartment neck dissection.
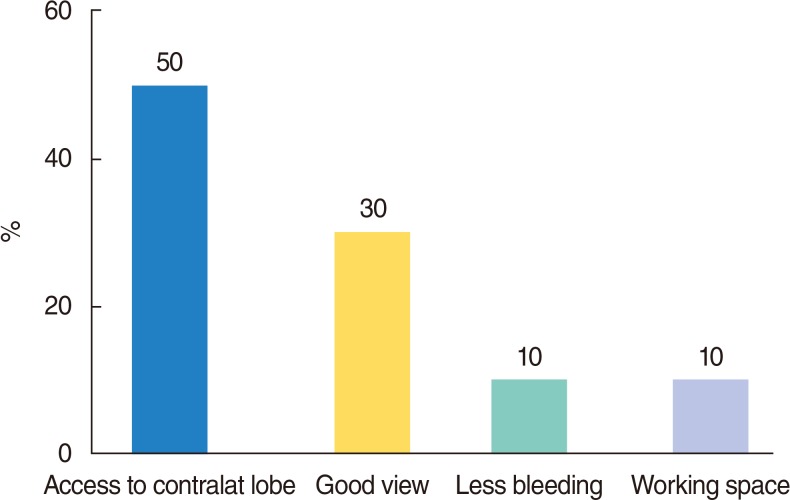
Fig. 5 Advantages of bilateral axillo-breast approach. Good view, good surgical view; Working space, enough working space.
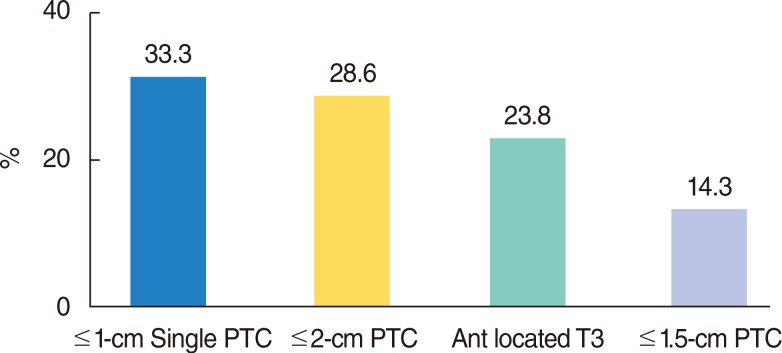
Fig. 6 Indications for endoscopic thyroidectomy in papillary thyroid cancer. PTC, papillary thyroid cancer.
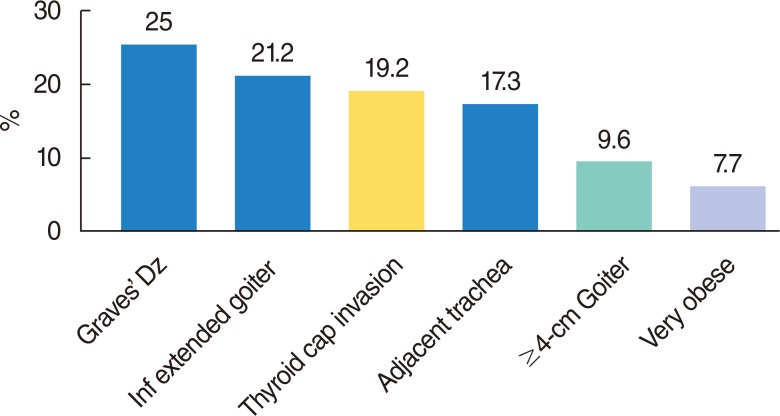
Fig. 7 Contraindications for endoscopic thyroidectomy. Graves' Dz, Graves' disease; Inf extended goiter, inferiorly extended thyroid goiter; Thyroid cap invasion, thyroid capsule invasion; Adjacent trachea, papillary thyroid cancer adjacent to the trachea.
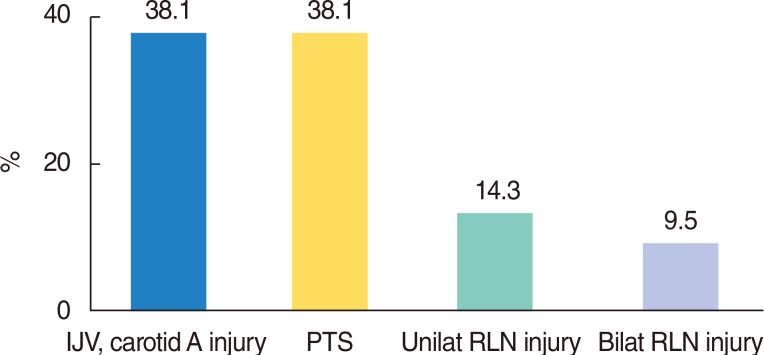
Fig. 8 Serious complications of endoscopic thyroidectomy. IJV, internal jugular vein; PTS, postthyroidectomy syndrome; RLN, recurrent laryngeal nerve.
Cited by 3 articles
-
Endoscopic Thyroidectomy Via the Cervico-axillary Approach for Thyroid Cancer: Initial Experience in a Single Institute
Jeong Shin An, Hyun Goo Kim, Se Hyun Paek, Jun Woo Lee, Juhyun Woo, Hyungju Kwon, Woosung Lim, Byung-In Moon, Nam Sun Paik
Korean J Endocr Surg. 2017;17(1):19-24. doi: 10.16956/kjes.2017.17.1.19.Robotic and Endoscopic Thyroid Surgery: Evolution and Advances
Kyung Tae, Yong Bae Ji, Chang Myeon Song, Junsun Ryu
Clin Exp Otorhinolaryngol. 2019;12(1):1-11. doi: 10.21053/ceo.2018.00766.Modified Transoral Endoscopic Thyroidectomy Technique Using Trapdoor Suspension Sutures
Su Il Kim, Hye Kyu Min, Dae Woong Kang, Soo Young Choi, Hee Jin Kang, Young Chan Lee, Young-Gyu Eun, Seong-Gyu Ko
Clin Exp Otorhinolaryngol. 2022;15(1):119-121. doi: 10.21053/ceo.2021.00101.
Reference
-
1. Gagner M. Endoscopic subtotal parathyroidectomy in patients with primary hyperparathyroidism. Br J Surg. 1996; 6. 83(6):875. PMID: 8696772.
Article2. Bae JS, Cho YU, Sung GY, Oh SJ, Jung EJ, Lee JB, et al. The current status of endoscopic thyroidectomy in Korea. Surg Laparosc Endosc Percutan Tech. 2008; 6. 18(3):231–235. PMID: 18574407.
Article3. Lee MC, Mo JA, Choi IJ, Lee BC, Lee GH. New endoscopic thyroidectomy via a unilateral axillo-breast approach with gas insufflation: Preliminary report. Head Neck. 2013; 4. 35(4):471–476. PMID: 22514023.
Article4. Yeung GH. Endoscopic thyroid surgery today: a diversity of surgical strategies. Thyroid. 2002; 8. 12(8):703–706. PMID: 12225638.
Article5. Kim JS, Kim KH, Ahn CH, Jeon HM, Kim EG, Jeon CS. A clinical analysis of gasless endoscopic thyroidectomy. Surg Laparosc Endosc Percutan Tech. 2001; 8. 11(4):268–272. PMID: 11525373.
Article6. Park YL, Han WK, Bae WG. 100 cases of endoscopic thyroidectomy: breast approach. Surg Laparosc Endosc Percutan Tech. 2003; 2. 13(1):20–25. PMID: 12598753.7. Yoon JH, Park CH, Chung WY. Gasless endoscopic thyroidectomy via an axillary approach: experience of 30 cases. Surg Laparosc Endosc Percutan Tech. 2006; 8. 16(4):226–231. PMID: 16921301.
Article8. Choe JH, Kim SW, Chung KW, Park KS, Han W, Noh DY, et al. Endoscopic thyroidectomy using a new bilateral axillo-breast approach. World J Surg. 2007; 3. 31(3):601–606. PMID: 17308853.
Article9. Koh YW, Kim JW, Lee SW, Choi EC. Endoscopic thyroidectomy via a unilateral axillo-breast approach without gas insufflation for unilateral benign thyroid lesions. Surg Endosc. 2009; 9. 23(9):2053–2060. PMID: 18528625.
Article10. Tae K, Ji YB, Cho SH, Kim KR, Kim DW, Kim DS. Initial experience with a gasless unilateral axillo-breast or axillary approach endoscopic thyroidectomy for papillary thyroid microcarcinoma: comparison with conventional open thyroidectomy. Surg Laparosc Endosc Percutan Tech. 2011; 6. 21(3):162–169. PMID: 21654299.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Current Status and the Perspectives of Nutrition Survey
- Clinical Analysis between the Endoscopic Thyroidectomy and the Open Thyroidectomy during the Same Period
- Comparison of Endoscopic Thyroidectomy versus Conventional Thyroidectomy in Patient Satisfaction with Cosmetic Result
- Anesthetic course and complications that were encountered during endoscopic thyroidectomy: A case report
- Comparison Study of Endoscopic Thyroidectomy Versus Robot-assisted Thyroidectomy by a Cervico-transaxillary Approach
