Sonoanatomic Variation of Pes Anserine Bursa
- Affiliations
-
- 1Department of Anesthesiology and Pain Medicine, Rasoul-Akram Medical Center, Tehran University of Medical Sciences, Tehran, Iran. borhanresearch@gmail.com
- KMID: 2074025
- DOI: http://doi.org/10.3344/kjp.2013.26.3.249
Abstract
- BACKGROUND
The pes anserine bursa lies beneath the pes anserine tendon, which is the insertional tendon of the sartorius, gracilis, and semitendinosus muscles on the medial side of the tibia, but it can lie in different sites in the medial knee. Accurate diagnosis of the position of the bursa is critical for diagnostic and therapeutic goals. The aim of this study was to evaluate sonoanatomic variations of the pes anserine bursa in the medial knee.
METHODS
One hundred seventy asymptomatic volunteers were enrolled in this study. Using ultrasound imaging (transverse approach, 7-13 MHz linear array probe) the sonoanatomic position of the pes anserine bursa and its relation to the pes anserine tendon were evaluated. Additionally, we evaluated the sonoanatomic variation of the saphenous nerve.
RESULTS
The position of the pes anserine bursa was between the medial collateral ligament and the pes anserine tendons in 21.2%/18.8% (males/females) of subjects; between the pes anserine tendons and the tibia in 67.1%/64.7% (m/f); and among the pes anserine tendons in 8.2%/12.9% (m/f). No significant differences in the position of the bursa existed between males and females. The saphenous nerve was found within the pes anserine tendons in 77.6%/74.1% (m/f) of subjects, but outside the pes anserine tendons in 18.8%/15.3% (m/f). Visibility of sonoanatomic structures was not related to either gender or BMI.
CONCLUSIONS
Ultrasound provides very accurate information about variations in the pes anserine bursa and the saphenous nerve. This suggests that our proposed ultrasound method can be a reliable guide to facilitate approaches to the medial knee for diagnostic and therapeutic objectives.
Keyword
Figure
-
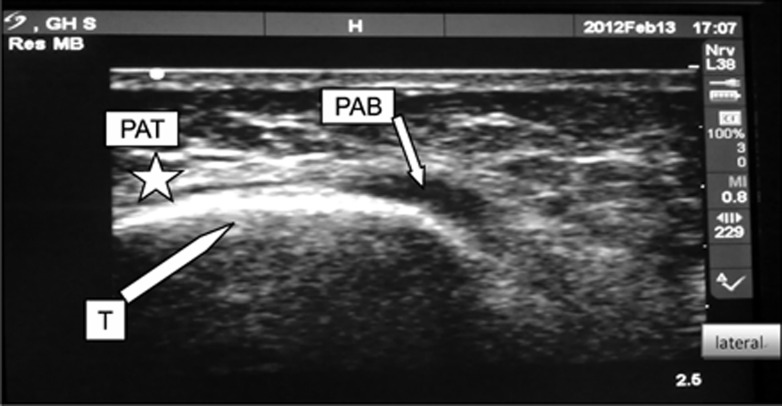
Fig. 1 Fluid filled pes anserine bursa (PAB) indicates the presence of bursitis. T: border of tibia, PAT: pes anserine tendons (asterisk).
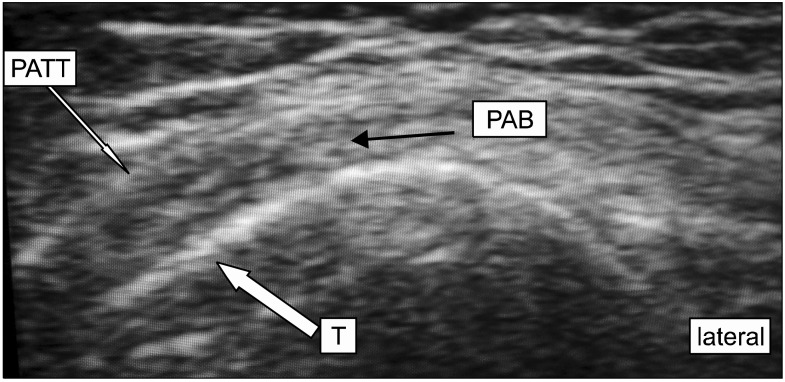
Fig. 2 Thickening of pes anserine tendons is shown. PATT: pes anserine tendon thickening, T: border of tibia, PAB: pes anserine bursa.
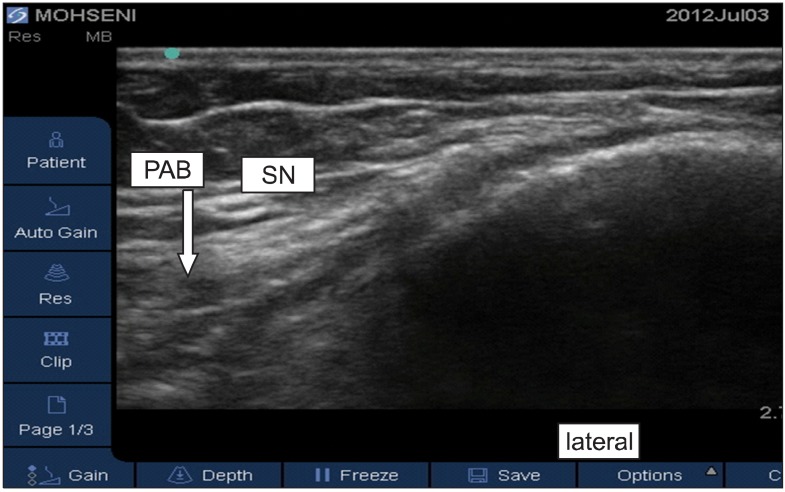
Fig. 3 Pes anserine bursa (PAB) is located between the pes anserine tendons and tibia. SN: saphenous nerve.
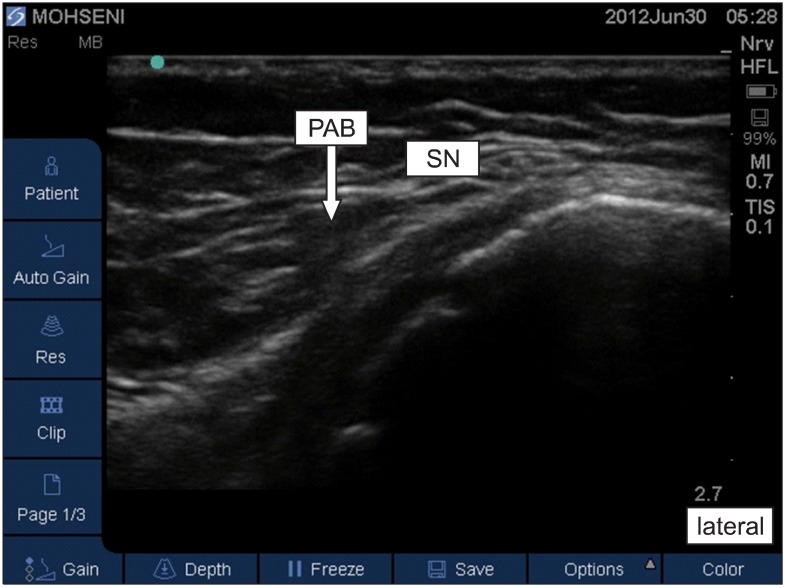
Fig. 4 Pes anserine bursa (PAB) lies under the pes anserine tendons. SN: saphenous nerve.
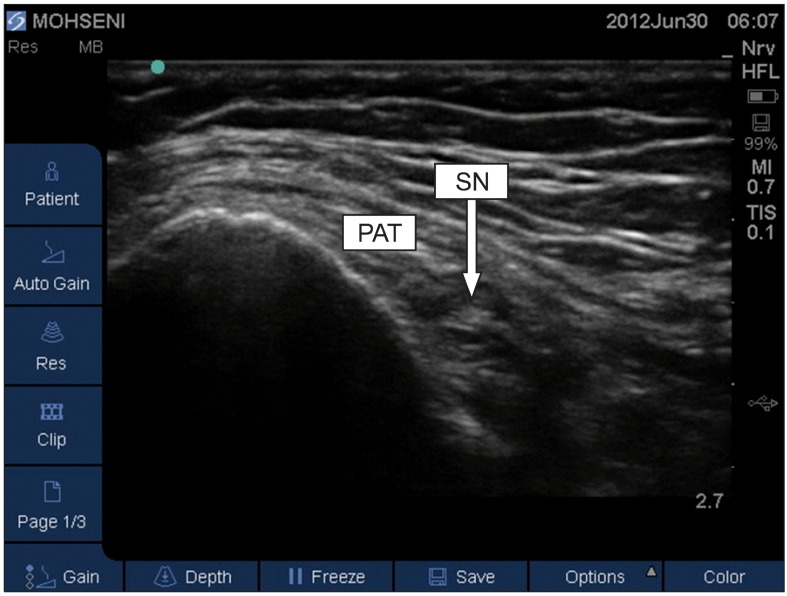
Fig. 5 Saphenous nerve lies between pes anserine tendons. PAT: pes anserine tendons, SN: saphenous nerve.

Fig. 6 Saphenous nerve is located outside of pes anserine tendons. PAT: pes anserine tendons, SN: saphenous nerve.
Cited by 1 articles
-
New insight into the vasto-adductor membrane for safer adductor canal blockade
Yanguk Heo, Miyoung Yang, Sung Min Nam, Hyun Seung Lee, Yeon-Dong Kim, Hyung-Sun Won
Korean J Pain. 2024;37(2):132-140. doi: 10.3344/kjp.23292.
Reference
-
1. Shrive NG, O'Connor JJ, Goodfellow JW. Load-bearing in the knee joint. Clin Orthop Relat Res. 1978; (131):279–287. PMID: 657636.
Article2. Jensen LK, Eenberg W. Occupation as a risk factor for knee disorders. Scand J Work Environ Health. 1996; 22:165–175. PMID: 8837261.
Article3. Mochizuki T, Akita K, Muneta T, Sato T. Pes anserinus: layered supportive structure on the medial side of the knee. Clin Anat. 2004; 17:50–54. PMID: 14695588.
Article4. Alvarez-Nemegyei J. Risk factors for pes anserinus tendinitis/bursitis syndrome: a case control study. J Clin Rheumatol. 2007; 13:63–65. PMID: 17414530.5. Chatra PS. Bursae around the knee joints. Indian J Radiol Imaging. 2012; 22:27–30. PMID: 22623812.
Article6. Kil HK, Cho JE, Kim WO, Koo BN, Han SW, Kim JY. Prepuncture ultrasound-measured distance: an accurate reflection of epidural depth in infants and small children. Reg Anesth Pain Med. 2007; 32:102–106. PMID: 17350519.
Article7. Wisniewski SJ, Smith J, Patterson DG, Carmichael SW, Pawlina W. Ultrasound-guided versus nonguided tibiotalar joint and sinus tarsi injections: a cadaveric study. PM R. 2010; 2:277–281. PMID: 20430329.
Article8. Reach JS, Easley ME, Chuckpaiwong B, Nunley JA 2nd. Accuracy of ultrasound guided injections in the foot and ankle. Foot Ankle Int. 2009; 30:239–242. PMID: 19321101.
Article9. Aaron DL, Patel A, Kayiaros S, Calfee R. Four common types of bursitis: diagnosis and management. J Am Acad Orthop Surg. 2011; 19:359–367. PMID: 21628647.
Article10. Calmbach WL, Hutchens M. Evaluation of patients presenting with knee pain: part II. Differential diagnosis. Am Fam Physician. 2003; 68:917–922. PMID: 13678140.11. Forbes JR, Helms CA, Janzen DL. Acute pes anserine bursitis: MR imaging. Radiology. 1995; 194:525–527. PMID: 7824735.
Article12. De Maeseneer M, Vanderdood K, Marcelis S, Shabana W, Osteaux M. Sonography of the medial and lateral tendons and ligaments of the knee: the use of bony landmarks as an easy method for identification. AJR Am J Roentgenol. 2002; 178:1437–1444. PMID: 12034613.
Article13. Butcher JD, Salzman KL, Lillegard WA. Lower extremity bursitis. Am Fam Physician. 1996; 53:2317–2324. PMID: 8638508.14. Rennie WJ, Saifuddin A. Pes anserine bursitis: incidence in symptomatic knees and clinical presentation. Skeletal Radiol. 2005; 34:395–398. PMID: 15940489.
Article15. Grover RP, Rakhra KS. Pes anserine bursitis - an extra-articular manifestation of gout. Bull NYU Hosp Jt Dis. 2010; 68:46–50. PMID: 20345364.16. Finnoff JT, Nutz DJ, Henning PT, Hollman JH, Smith J. Accuracy of ultrasound-guided versus unguided pes anserinus bursa injections. PM R. 2010; 2:732–739. PMID: 20598959.
Article17. Valley VT, Shermer CD. Use of musculoskeletal ultrasonography in the diagnosis of pes anserine tendinitis: a case report. J Emerg Med. 2001; 20:43–45. PMID: 11165837.
Article18. Curtiss HM, Finnoff JT, Peck E, Hollman J, Muir J, Smith J. Accuracy of ultrasound-guided and palpation-guided knee injections by an experienced and less-experienced injector using a superolateral approach: a cadaveric study. PM R. 2011; 3:507–515. PMID: 21665162.
Article19. Gilliland CA, Salazar LD, Borchers JR. Ultrasound versus anatomic guidance for intra-articular and periarticular injection: a systematic review. Phys Sportsmed. 2011; 39:121–131. PMID: 22030948.
Article20. Epis O, Iagnocco A, Meenagh G, Riente L, Delle Sedie A, Filippucci E, et al. Ultrasound imaging for the rheumatologist. XVI. Ultrasound-guided procedures. Clin Exp Rheumatol. 2008; 26:515–518. PMID: 18799078.21. Hemler DE, Ward WK, Karstetter KW, Bryant PM. Saphenous nerve entrapment caused by pes anserine bursitis mimicking stress fracture of the tibia. Arch Phys Med Rehabil. 1991; 72:336–337. PMID: 2009053.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Tenosynovial Giant Cell Tumor of the Pes Anserine Bursa with Bone Marrow Extension into the Tibia: A Case Report
- Pes anserinus and anserine bursa: anatomical study
- Two Cases of Traumatic Anserine Folliculosis
- A Case of Traumatic Anserine Folliculosis
- Correlation between Ultrasonographic Findings and The Response to Corticosteroid Injection in Pes Anserinus Tendinobursitis Syndrome in Knee Osteoarthritis Patients
