Pes anserinus and anserine bursa: anatomical study
- Affiliations
-
- 1Department of Anatomy, Konyang University College of Medicine, Daejeon, Korea.
- 2Department of Anatomy, Catholic Institute for Applied Anatomy, The Catholic University of Korea College of Medicine, Seoul, Korea.
- 3College of Natural Sciences, Soonchunhyang University, Cheonan, Korea.
- 4Department of Anatomy, Chung-Ang University College of Medicine, Seoul, Korea. hsh@catholic.ac.kr
- KMID: 1882583
- DOI: http://doi.org/10.5115/acb.2014.47.2.127
Abstract
- This study investigated the boundary of anserine bursa with the recommended injection site and shape on the insertion area of pes anserinus (PA), with the aim of improving clinical practice. Eighty six legs from 45 Korean cadavers were investigated. The mixed gelatin solution was injected to identify the shape of anserine bursa, and then the insertion site of the PA tendons was exposed completely and carefully dissected to identify the shape of the PA. The sartorius was inserted into the superficial layer and gracilis, and the semitendinosus was inserted into the deep layer on the medial surface of the tibia. The number of the semitendinosus tendons at the insertion site varied: 1 in 66% of specimens, 2 in 31%, and 3 in 3%. The gracilis and semitendinosus tendons were connected to the deep fascia of leg. Overall, the shape of the anserine bursa was irregularly circular. Most of the anserine bursa specimens reached the proximal line of the tibia, and some of the specimens reached above the proximal line of the tibia. In the medial view of the tibia, the anserine bursa was located posteriorly and superiorly from the tibia's midline, and it followed the lines of the sartorius muscle. The injection site for anserine bursa should be carried out at 20degrees from the vertical line medially and inferiorly, 15 or 20 mm deeply, and at the point of about 20 mm medial and 12 mm superior from inferomedial point of tibial tuberosity.
Keyword
Figure
-
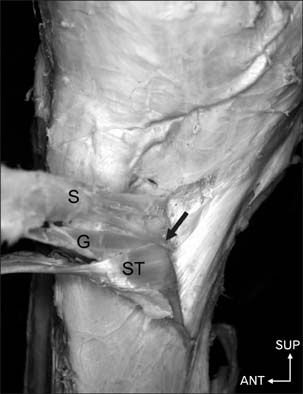
Fig. 1 Sartorius tendon variation at the insertion site. Some parts of the sartorius tendon were inserted into deeper layer than the gracilis and semitendinosus tendons (arrow). ANT, anterior, G, gracilis; S, Sartorius; ST, semitendinosus; SUP, superior.

Fig. 2 Typical insertion site of the pes anserinus. Dotted line denotes the inferior border of the sartorius muscle. (A) Semitendinosus was attached to the inner space of the inferior borders of sartorius. (B) Semitendinosus was attached inferior to the Sartorius. ANT, anterior; G, gracilis; S, Sartorius; ST, semitendinosus; SUP, superior.

Fig. 3 Variation of the semitendinosus tendon at the insertion site. (A) The semitendinosus tendon was divided into two. (B) The semitendinosus tendon was divided into three. ANT, anterior; G, gracilis; POST, posterior; S, Sartorius; ST, semitendinosus; SUP, superior.

Fig. 4 The injection method in the anserine bursa. The injection-needle was positioned at 20° from the vertical line medially and inferiorly, 20.0±2.0 mm medial and 12.0±3.0 mm superior from the inferomedial point of the tibial tuberosity. SUP, superior; MED, medial.

Fig. 5 The anserine bursa revealed by injection of gelatin containing blue ink. IB, infrapatellar branch; S, Sartorius; SN, saphenous nerve; SV, saphenous vein; ANT, anterior; SUP, superior.
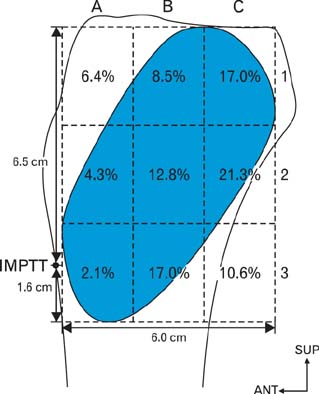
Fig. 6 The distribution of nerves and vessels in the anserine bursa. The proximal line of AB from inferomedial point of tibial tuberosity (IMPTT) was 16.0±5.0 mm, the distal line of AB from IMPTT was 65.0±7.0 mm, the posterior line of AB from IMPTT was 60.0±7.6 mm. ANT, anterior; SUP, superior.
Cited by 1 articles
-
Dimensions of pes anserinus of the lower extremity, an anatomical study with its surgical implications
Rajanigandha Vadgaonkar, M.D. Prameela, Chettiar Ganesh Kumar, Vandana Blossom, Mamatha Tonse, B.V. Murlimanju, Mangala M. Pai, Latha V. Prabhu
Anat Cell Biol. 2021;54(2):178-183. doi: 10.5115/acb.20.275.
Reference
-
1. Candal-Couto JJ, Deehan DJ. The accessory bands of Gracilis and Semitendinosus: an anatomical study. Knee. 2003; 10:325–328.2. Mochizuki T, Akita K, Muneta T, Sato T. Pes anserinus: layered supportive structure on the medial side of the knee. Clin Anat. 2004; 17:50–54.3. Ivey M, Prud'homme J. Anatomic variations of the pes anserinus: a cadaver study. Orthopedics. 1993; 16:601–606.4. Gnanadesigan N, Smith RL. Knee pain: osteoarthritis or anserine bursitis? J Am Med Dir Assoc. 2003; 4:164–166.5. Yoon HS, Kim SE, Suh YR, Seo YI, Kim HA. Correlation between ultrasonographic findings and the response to corticosteroid injection in pes anserinus tendinobursitis syndrome in knee osteoarthritis patients. J Korean Med Sci. 2005; 20:109–112.6. Brookler MI, Mongan ES. Anserina bursitis. A treatable cause of knee pain in patients with degenerative arthritis. Calif Med. 1973; 119:8–10.7. Clapp A, Trecek J, Joyce M, Sundaram M. Radiologic case study. Pes anserine bursitis. Orthopedics. 2008; 31:306407–408.8. Osman MK, Irwin GJ, Huntley JS. Swelling around a child's knee. Clin Anat. 2011; 24:914–917.9. Helfenstein M Jr, Kuromoto J. Anserine syndrome. Rev Bras Reumatol. 2010; 50:313–327.10. Finnoff JT, Nutz DJ, Henning PT, Hollman JH, Smith J. Accuracy of ultrasound-guided versus unguided pes anserinus bursa injections. PM R. 2010; 2:732–739.11. Beals TC, Harryman DT 2nd, Lazarus MD. Useful boundaries of the subacromial bursa. Arthroscopy. 1998; 14:465–470.12. Bureau NJ, Dussault RG, Keats TE. Imaging of bursae around the shoulder joint. Skeletal Radiol. 1996; 25:513–517.13. Dunn T, Heller CA, McCarthy SW, Dos Remedios C. Anatomical study of the "trochanteric bursa". Clin Anat. 2003; 16:233–240.14. Kassarjian A, Llopis E, Schwartz RB, Bencardino JT. Obturator externus bursa: prevalence of communication with the hip joint and associated intra-articular findings in 200 consecutive hip MR arthrograms. Eur Radiol. 2009; 19:2779–2782.15. Robinson P, White LM, Agur A, Wunder J, Bell RS. Obturator externus bursa: anatomic origin and MR imaging features of pathologic involvement. Radiology. 2003; 228:230–234.16. Sardelli M, Burks RT. Distances to the subacromial bursa from 3 different injection sites as measured arthroscopically. Arthroscopy. 2008; 24:992–996.17. Schraner AB, Major NM. MR imaging of the subcoracoid bursa. AJR Am J Roentgenol. 1999; 172:1567–1571.18. Strizak AM, Danzig L, Jackson DW, Resnick D, Staple T. Subacromial bursography. An anatomical and clinical study. J Bone Joint Surg Am. 1982; 64:196–201.19. Woodley SJ, Mercer SR, Nicholson HD. Morphology of the bursae associated with the greater trochanter of the femur. J Bone Joint Surg Am. 2008; 90:284–294.20. LaPrade RF, Engebretsen AH, Ly TV, Johansen S, Wentorf FA, Engebretsen L. The anatomy of the medial part of the knee. J Bone Joint Surg Am. 2007; 89:2000–2010.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Sonoanatomic Variation of Pes Anserine Bursa
- Tenosynovial Giant Cell Tumor of the Pes Anserine Bursa with Bone Marrow Extension into the Tibia: A Case Report
- Correlation between Ultrasonographic Findings and The Response to Corticosteroid Injection in Pes Anserinus Tendinobursitis Syndrome in Knee Osteoarthritis Patients
- Snapping Pes Anserinus Caused By Gracilis Tendon: A New Mechanism Proposed by Dynamic Knee Ultrasonography
- Clinical Study of Operative Treatment of Medical Collateral Ligamentous Injuries of the Knee Joint
