Evaluation of a Chest Circumference-Adapted Protocol for Low-Dose 128-Slice Coronary CT Angiography with Prospective Electrocardiogram Triggering
- Affiliations
-
- 1Department of Radiology, Lishui Central Hospital, The Fifth Affiliated Hospital of Wenzhou Medical College, Lishui, Zhejiang 323000, China. jjstcty@sina.com
- KMID: 2069981
- DOI: http://doi.org/10.3348/kjr.2015.16.1.13
Abstract
OBJECTIVE
To assess the effect of chest circumference-adapted scanning protocol on radiation exposure and image quality in patients undergoing prospective electrocardiogram (ECG)-triggered coronary CT angiography (CCTA).
MATERIALS AND METHODS
One hundred-eighty-five consecutive patients, who had undergone prospective ECG triggering CCTA with a 128-slice CT, were included in the present study. Nipple-level chest circumference, body weight and height were measured before CT examinations. Patients were divided into four groups based on kV/ref.mAs = 100/200, 100/250, 120/200, and 120/250, when patient's chest circumference was < or = 85.0 (n = 56), 85.0-90.0 (n = 53), 90.0-95.0 (n = 44), and > 95.0 (n = 32), respectively. Image quality per-segment was independently assessed by two experienced observers. Image noise and attenuation were also measured. Signal-to-noise ratio (SNR) and contrast-to-noise ratio (CNR) were calculated. The effective radiation dose was calculated using CT dose volume index and the dose-length product.
RESULTS
A significant correlation was observed between patients' chest circumference and body mass index (r = 0.762, p < 0.001). Chest circumference ranged from 74 to 105 cm, and the mean effective radiation dose was 1.9-3.8 mSv. Diagnostic image quality was obtained in 98.5% (2440/2478) of all evaluated coronary segments without any significant differences among the four groups (p = 0.650). No significant difference in image noise was observed among the four groups (p = 0.439), thus supporting the validity of the chest circumference-adapted scanning protocol. However, vessel attenuation, SNR and CNR were significantly higher in the 100 kV groups than in the 120 kV groups (p < 0.05).
CONCLUSION
A measure of chest circumference can be used to adapt tube voltage and current for individualized radiation dose control, with resultant similar image noise and sustained diagnostic image quality.
Keyword
MeSH Terms
Figure
-

Fig. 1 Linear regression plot showing significant correlation between chest circumference and body mass index (r = 0.762, p < 0.001).
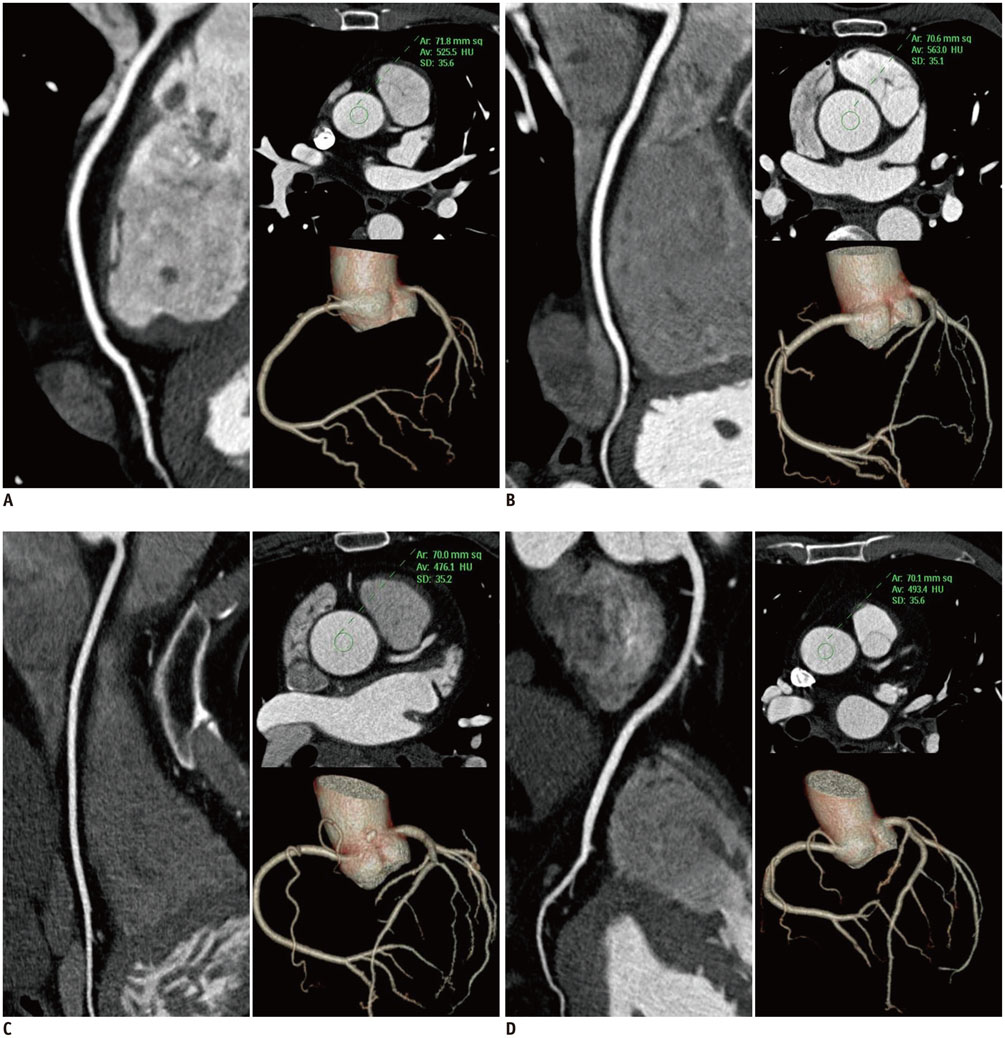
Fig. 2 Curved-planar reconstruction of right coronary artery and volume-rendered trees demonstrating image quality of four CCTA protocols. A. Tube voltage 100 kV, tube current 200 mAs. B. Tube voltage 100 kV, tube current 250 mAs. C. Tube voltage 120 kV, tube current 200 mAs. D. Tube voltage 120 kV, tube current 250 mAs. ROI was placed at root of ascending aorta and image noise was similar in four groups, while image quality of coronary segments remained diagnostic. CCTA = coronary CT angiography, ROI = region of interest

Fig. 3 77-year-old man with BMI of 23.0 and chest circumference of 84.0 cm. Axial CT images obtained at 100 kV and 200 mAs show ascending aorta with image noise of 36 HU and vessel attenuation of 611 HU. BMI = body mass index, HU = Hounsfield unit
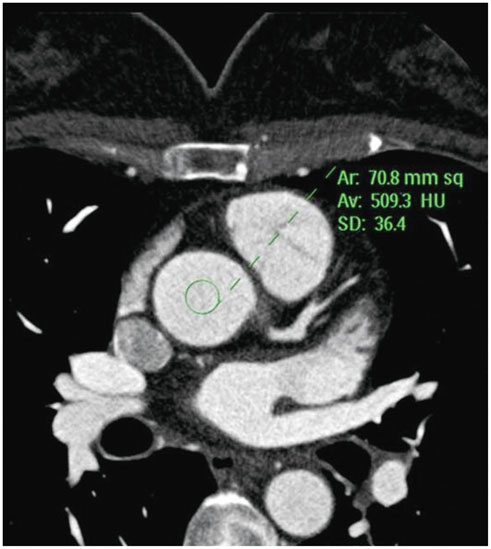
Fig. 4 45-year-old woman with BMI of 23.1 and chest circumference of 94.0 cm. Axial CT images obtained at 120 kV and 200 mAs show ascending aorta with image noise of 36.4 HU and vessel attenuation of 509.3 HU. This female patient had same BMI, but larger chest circumference, than male patient represented in Figure 3. Image noise was similar when chest circumference-adapted scanning protocol was used. BMI = body mass index, HU = Hounsfield unit
Reference
-
1. Motoyama S, Anno H, Sarai M, Sato T, Sanda Y, Ozaki Y, et al. Noninvasive coronary angiography with a prototype 256-row area detector computed tomography system: comparison with conventional invasive coronary angiography. J Am Coll Cardiol. 2008; 51:773–775.2. Miller JM, Rochitte CE, Dewey M, Arbab-Zadeh A, Niinuma H, Gottlieb I, et al. Diagnostic performance of coronary angiography by 64-row CT. N Engl J Med. 2008; 359:2324–2336.3. Rybicki FJ, Otero HJ, Steigner ML, Vorobiof G, Nallamshetty L, Mitsouras D, et al. Initial evaluation of coronary images from 320-detector row computed tomography. Int J Cardiovasc Imaging. 2008; 24:535–546.4. Einstein AJ, Henzlova MJ, Rajagopalan S. Estimating risk of cancer associated with radiation exposure from 64-slice computed tomography coronary angiography. JAMA. 2007; 298:317–323.5. Hausleiter J, Meyer T, Hermann F, Hadamitzky M, Krebs M, Gerber TC, et al. Estimated radiation dose associated with cardiac CT angiography. JAMA. 2009; 301:500–507.6. Achenbach S, Goroll T, Seltmann M, Pflederer T, Anders K, Ropers D, et al. Detection of coronary artery stenoses by lowdose, prospectively ECG-triggered, high-pitch spiral coronary CT angiography. JACC Cardiovasc Imaging. 2011; 4:328–337.7. Hong YJ, Kim SJ, Lee SM, Min PK, Yoon YW, Lee BK, et al. Low-dose coronary computed tomography angiography using prospective ECG-triggering compared to invasive coronary angiography. Int J Cardiovasc Imaging. 2011; 27:425–431.8. Hosch W, Heye T, Schulz F, Lehrke S, Schlieter M, Giannitsis E, et al. Image quality and radiation dose in 256-slice cardiac computed tomography: comparison of prospective versus retrospective image acquisition protocols. Eur J Radiol. 2011; 80:127–135.9. Herzog BA, Husmann L, Valenta I, Tay FM, Burkhard N, Gaemperli O, et al. Determinants of vessel contrast in BMIadapted low dose CT coronary angiography with prospective ECG-triggering. Int J Cardiovasc Imaging. 2009; 25:625–630.10. Hosch W, Stiller W, Mueller D, Gitsioudis G, Welzel J, Dadrich M, et al. Reduction of radiation exposure and improvement of image quality with BMI-adapted prospective cardiac computed tomography and iterative reconstruction. Eur J Radiol. 2012; 81:3568–3576.11. Ghoshhajra BB, Engel LC, Major GP, Verdini D, Sidhu M, Károlyi M, et al. Direct chest area measurement: a potential anthropometric replacement for BMI to inform cardiac CT dose parameters? J Cardiovasc Comput Tomogr. 2011; 5:240–246.12. Valentin J. International Commission on Radiation Protection. Managing patient dose in multi-detector computed tomography (MDCT). ICRP Publication 102. Ann ICRP. 2007; 37:1–79. iii.13. Austen WG, Edwards JE, Frye RL, Gensini GG, Gott VL, Griffith LS, et al. A reporting system on patients evaluated for coronary artery disease. Report of the Ad Hoc Committee for Grading of Coronary Artery Disease, Council on Cardiovascular Surgery, American Heart Association. Circulation. 1975; 51:4 Suppl. 5–40.14. Matsubara K, Koshida K, Suzuki M, Shimono T, Yamamoto T, Matsui O. Effective dose evaluation of multidetector CT examinations: influence of the ICRP recommendation in 2007. Eur Radiol. 2009; 19:2855–2861.15. Neefjes LA, Dharampal AS, Rossi A, Nieman K, Weustink AC, Dijkshoorn ML, et al. Image quality and radiation exposure using different low-dose scan protocols in dual-source CT coronary angiography: randomized study. Radiology. 2011; 261:779–786.16. Hoang JK, Hurwitz LM, Boll DT. Optimization of tube current in coronary multidetector computed tomography angiography: assessment of a standardized method to individualize current selection based on body habitus. J Comput Assist Tomogr. 2009; 33:498–504.17. Bischoff B, Hein F, Meyer T, Hadamitzky M, Martinoff S, Schömig A, et al. Impact of a reduced tube voltage on CT angiography and radiation dose: results of the PROTECTION I study. JACC Cardiovasc Imaging. 2009; 2:940–946.18. Feuchtner GM, Jodocy D, Klauser A, Haberfellner B, Aglan I, Spoeck A, et al. Radiation dose reduction by using 100-kV tube voltage in cardiac 64-slice computed tomography: a comparative study. Eur J Radiol. 2010; 75:e51–e56.19. Leipsic J, Labounty TM, Heilbron B, Min JK, Mancini GB, Lin FY, et al. Estimated radiation dose reduction using adaptive statistical iterative reconstruction in coronary CT angiography: the ERASIR study. AJR Am J Roentgenol. 2010; 195:655–660.20. Menke J. Comparison of different body size parameters for individual dose adaptation in body CT of adults. Radiology. 2005; 236:565–571.21. Leschka S, Stolzmann P, Schmid FT, Scheffel H, Stinn B, Marincek B, et al. Low kilovoltage cardiac dual-source CT: attenuation, noise, and radiation dose. Eur Radiol. 2008; 18:1809–1817.22. Pflederer T, Rudofsky L, Ropers D, Bachmann S, Marwan M, Daniel WG, et al. Image quality in a low radiation exposure protocol for retrospectively ECG-gated coronary CT angiography. AJR Am J Roentgenol. 2009; 192:1045–1050.23. Nakayama Y, Awai K, Funama Y, Hatemura M, Imuta M, Nakaura T, et al. Abdominal CT with low tube voltage: preliminary observations about radiation dose, contrast enhancement, image quality, and noise. Radiology. 2005; 237:945–951.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Utility of Coronary CT Angiography with Low-dose Chest CT in the Evaluation of Patients with Atypical Chest Pain: A Preliminary Report
- Noninvasive Detection of Coronary Atherosclerotic Plaques and Assessment of Stenosis Degree at Multidetector CT Coronary Angiography
- Coronary Artery Anomalies: Assessment with Electrocardiography-Gated Multidetector-Row CT at a Single Center in Korea
- Diagnostic accuracy of 64-slice multi-detector CT coronary angiography in the evaluation of coronary artery disease
- The Diagnostic Accuracy of the 64-slice Multi-detector CT Coronary Angiography for the Assessment of Coronary Artery Stenosis in Symptomatic Patients
