Huge Intramural Hematoma in a Thrombosed Middle Cerebral Artery Aneurysm: A Case Report
- Affiliations
-
- 1Department of Neurosurgery, Pusan National University Yangsan Hospital, Pusan National University School of Medicine, Yangsan, Korea. md@medimail.com
- 2Department of Radiology, Pusan National University Yangsan Hospital, Pusan National University School of Medicine, Yangsan, Korea.
- KMID: 2069249
- DOI: http://doi.org/10.7461/jcen.2015.17.3.234
Abstract
- We describe a case of a huge intramural hematoma in a thrombosed middle cerebral artery aneurysm. A 47-year-old female patient with liver cirrhosis and thrombocytopenia presented to the neurosurgical unit with a 5-day history of headache and cognitive dysfunction. Magnetic resonance imaging and computed tomography of the brain showed a thrombosed aneurysm located in the right middle cerebral artery with a posteriorly located huge intramural hematoma mimicking an intracerebral hematoma. Imaging studies and cerebrospinal fluid analysis showed no evidence of subarachnoid hemorrhage. Angiography showed a partially thrombosed aneurysm at the origin of the right anterior temporal artery and an incidental aneurysm at the bifurcation of the right middle cerebral artery. Both aneurysms were embolized by coiling. After embolization, the thrombosed aneurysmal sac and intramural hematoma had decreased in size 4 days later and almost completely disappeared 8 months later. This is the first reported case of a nondissecting, nonfusiform aneurysm with a huge intramural hematoma, unlike that of a dissecting aneurysm.
MeSH Terms
Figure
-
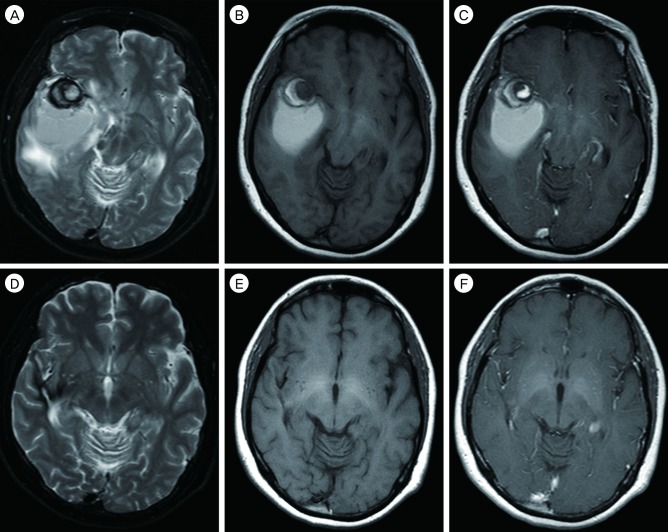
Fig. 1 Initial T1-weighted axial image shows the target-like thrombosed aneurysm in the right anterior sylvian fissure (B). Another ovoid high signal intensity suggests hematoma surrounded by the posterior aspect of the aneurysm. T2-weighted axial image also shows the thrombosed aneurysm and posteriorly located hematoma with a surrounding dark line (A). The posteriorly located hematoma differs in signal intensity from the thrombosed aneurysm on T1- and T2-weighted images, i.e., the posterior hematoma shows homogeneous high signal intensity, whereas the thrombosed portion of the aneurysm shows intermediate and inhomogeneous high signal intensity on T1- and T2-weighted images (A, B). Gd-enhanced axial image shows no definite enhancement of the lesions (C). After one year, MR of the brain shows almost resorption state of the hematoma in the right temporal lobe.(D-F).
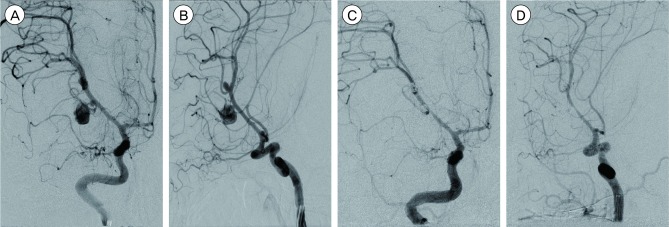
Fig. 2 Digital subtraction angiography was performed and two unruptured aneurysms were found in the right middle cerebral artery. (A, B) Surgical intervention was not performed due to continued thrombocytopenia. Instead, coil embolization followed immediately. After embolization of two aneurysms, follow-up angiography shows faint staining of the contrast
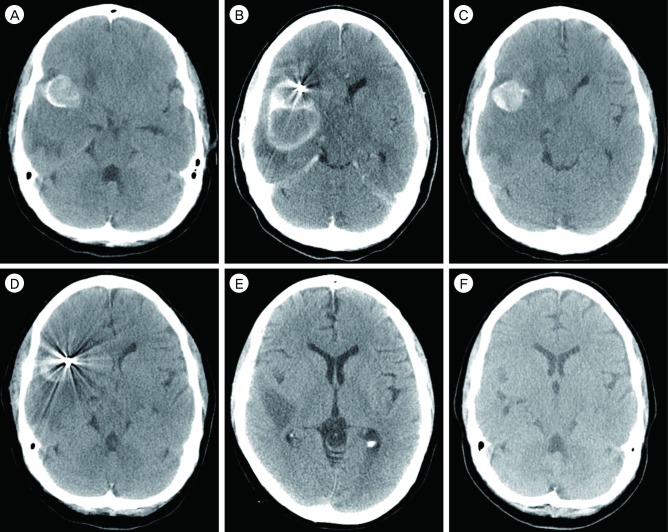
Fig. 3 On precontrast CT scan (A), the thrombosed aneurysm shows a high attenuating wall. The posteriorly located hematoma abuts the aneurysm sac. The hematoma also differs from the high attenuating aneurysm wall in density. Follow-up brain CT was performed immediately after coil embolization. Capsular enhancement is seen not only in the aneurysm sac but also in the posterior hematoma (B). (C-E) and F are CT images of the brain at POD 4 days, 11 days, 1 month, and 5 months. The aneurysm sac and hematoma had decreased in size 4 days after coil embolization (C-E) and almost disappeared 4 months later (F).
Cited by 1 articles
-
Staged hybrid treatment for giant thrombosed fusiform aneurysm
Yunho Noh, Sung Ho Lee, Seok Mann Yoon, In Hag Song, Jae Sang Oh
J Cerebrovasc Endovasc Neurosurg. 2021;23(4):359-364. doi: 10.7461/jcen.2021.E2021.06.004.
Reference
-
1. El Beltagy M, Muroi C, Imhof HG, Yonekawa Y. Peripheral large or giant fusiform middle cerebral artery aneurysms: report of our experience and review of literature. Acta Neurochir Suppl. 2008; 103:37–44. PMID: 18496943.2. Horie N, Takahashi N, Furuichi S, Mori K, Onizuka M, Tsutsumi K, et al. Giant fusiform aneurysms in the middle cerebral artery presenting with hemorrhages of different origins. Report of three cases and review of the literature. J Neurosurg. 2003; 8. 99(2):391–396. PMID: 12924715.3. Krings T, Choi IS. The many faces of intracranial arterial dissections. Interv Neuroradiol. 2010; 6. 16(2):151–160. PMID: 20642889.
Article4. Krings T, Lasjaunias PL, Geibprasert S, Pereira V, Hans FJ. The aneurysmal wall. The key to a subclassification of intracranial arterial aneurysm vasculopathies? Interv Neuroradiol. 2008; 9. 14(Suppl 1):39–47. PMID: 20557772.5. Krings T, Piske RL, Lasjaunias PL. Intracranial arterial aneurysm vasculopathies: targeting the outer vessel wall. Neuroradiology. 2005; 12. 47(12):931–937. PMID: 16136262.
Article6. Mrak G, Paladino J, Stambolija V, Nemir J, Sekhar LN. Treatment of giant and large fusiform middle cerebral artery aneurysms with excision and interposition radial artery graft in a 4-year-old child: case report. Neurosurgery. 2014; 3. 10(Suppl 1):E172–E177. discussion E177PMID: 24509498.
Article7. Nagahiro S, Takada A, Goto S, Kai Y, Ushio Y. Thrombosed growing giant aneurysms of the vertebral artery: growth mechanism and management. J Neurosurg. 1995; 5. 82(5):796–801. PMID: 7714605.
Article8. Sagoh M, Hirose Y, Murakami H, Akaji K, Katayama M, Hayashi T. Late hemorrhage from persistent pseudoaneurysm in vertebral artery dissection presenting with ischemia: case report. Surg Neurol. 1999; 11. 52(5):480–483. discussion 483-4. PMID: 10595768.
Article9. Yasui T, Sakamoto H, Kishi H, Komiyama M, Iwai Y, Yamanaka K, et al. Rupture mechanism of a thrombosed slow-growing giant aneurysm of the vertebral artery-case report. Neurol Med Chir (Tokyo). 1998; 12. 38(12):860–864. PMID: 10063360.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Subdural Hematoma Due to Ruptured Intracerebral Aneurysm
- Intracranial Mycotic Aneurysm: Case Report
- Subarachnoid Hemorrhage Due to a Ruptured Middle Cerebral Artery Bifurcation Aneurysm Superimposed by an Idiopathic Intracerebral Hematoma
- Duplication of the Middle Cerebral Artery: Case Report
- Thrombosed Large Middle Cerebral Artery Aneurysm Mimicking an Intra-Axial Brain Tumor: Case Report and Review of Literature
