Synchronous Triple Primary Lung Cancer: A Rare Case with Radiologic-Pathologic Correlation
- Affiliations
-
- 1Department of Radiology and the Research Institute of Radiological Science, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Korea. park_chulhwan@yuhs.ac
- 2Department of Thoracic and Cardiovascular Surgery, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Korea.
- 3Department of Pathology, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 2068712
- DOI: http://doi.org/10.3348/jksr.2015.73.4.225
Abstract
- Synchronous multiple primary lung cancer is uncommon. They present at the same time, but are distinct and have different histologic features. Synchronous triple primary lung cancer is rare and only few cases have been reported previously. We described a case of synchronous triple primary lung cancers in an asymptomatic 64-year-old man that showed different radiologic features of lung tumors on chest computed tomography images. Anatomical resection and histological analysis revealed 3 different types of lung carcinoma with radiologic-pathologic correlation.
MeSH Terms
Figure
-

Fig. 1 A rounded solid nodule in the right lower lobe superior segment of the lung (lesion 1). A. An initial axial computed tomography (CT) scan shows a 0.7 mm solid nodule (arrow). B. A 9-month follow-up CT image shows an enlargement of the nodule in right lower lobe (RLL) superior segment to 1.8 cm with evidence of lobulation and spicule formation (arrow). C. A positron emission tomography-CT image shows 18F-fluorodeoxyglucose uptake (standardized uptake value = 7.4) in lesion 1 (arrow). D. Macroscopic examination of the superior segment of the RLL of the lung reveals a 1.6 cm solid mass (arrow). E. This lesion was confirmed as adenocarcinoma composed of solid and micropapillary patterns (× 200).

Fig. 2 A ground-glass opacity nodule in the right lower lobe (RLL) lateral basal segment of the lung (lesion 2). A. On an axial computed tomography (CT) scan, a 1.4 cm subsolid nodule (arrow) is detected at the basal segment of the RLL. B. There is no change in the lesion size on a 9-month follow-up CT image (arrow). C. A positron emission tomography-CT image shows that there was no focal 18F-fluorodeoxyglucose uptake by the nodule (arrow). D. A gross image in the lateral basal segment of the RLL of the lung reveals a 1.0 cm ill-defined nodule with discoloration (arrow). E. Lesion 2 was confirmed as adenocarcinoma, acinar predominant type (× 200).
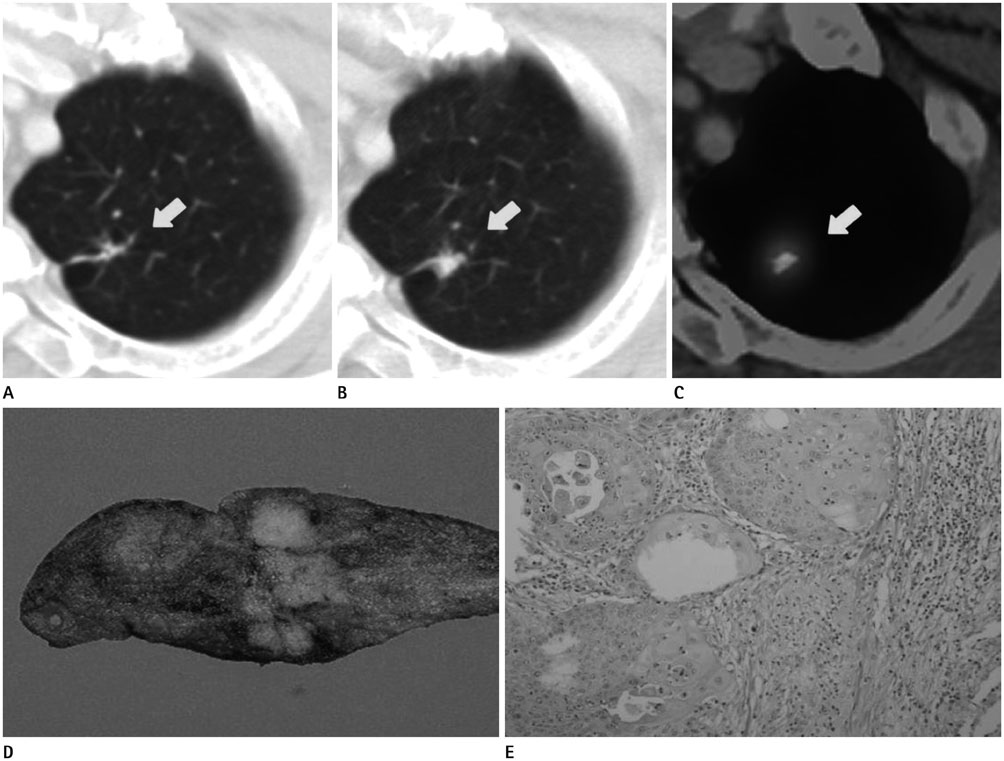
Fig. 3 A cavitary nodular lesion in the left upper lobe (LUL) of the lung (lesion 3). A. A 1.2 cm irregular-shaped cavitary nodular lesion without calcification (arrow) is located in LUL on an axial computed tomography (CT) image. B. CT images taken at a 9-month follow-up indicate that lesion size is increased to 1.4 cm (arrow). C. A positron emission tomography-CT image shows focal 18F-fluorodeoxyglucose uptake (standardized uptake value = 3.8) in this lesion (arrow). D. On gross findings, a solid mass in the wedge resection specimen of the LUL of the lung extends to the resection margin. E. This lesion was confirmed as moderately differentiated squamous cell carcinoma (× 200).
Reference
-
1. Martini N, Melamed MR. Multiple primary lung cancers. J Thorac Cardiovasc Surg. 1975; 70:606–612.2. Flynn MJ, Rassl D, El Shahira A, Higgins B, Barnard S. Metachronous and synchronous lung tumors: five malignant lung pathologies in 1 patient during 7 years. Ann Thorac Surg. 2004; 78:2154–2155.3. Tokuchi Y, Kamachi M, Harada M, Hasegawa M, Mishina T, Yamashiro K, et al. Synchronous triple lung cancers after treatment for non-Hodgkin's lymphoma: metachronous quadruple cancers. Intern Med. 2003; 42:1031–1034.4. Froio E, D'Adda T, Fellegara G, Ampollini L, Carbognani P, Rindi G. Three different synchronous primary lung tumours: a case report with extensive genetic analysis and review of the literature. Lung Cancer. 2008; 59:395–402.5. Yoon HJ, Lee HY, Han J, Choi YL. Synchronous triple primary lung cancers: a case report. Korean J Radiol. 2014; 15:646–650.6. Chang YL, Wu CT, Lee YC. Surgical treatment of synchronous multiple primary lung cancers: experience of 92 patients. J Thorac Cardiovasc Surg. 2007; 134:630–637.7. Zwirewich CV, Vedal S, Miller RR, Müller NL. Solitary pulmonary nodule: high-resolution CT and radiologic-pathologic correlation. Radiology. 1991; 179:469–476.8. Travis WD, Brambilla E, Noguchi M, Nicholson AG, Geisinger KR, Yatabe Y, et al. International association for the study of lung cancer/american thoracic society/european respiratory society international multidisciplinary classification of lung adenocarcinoma. J Thorac Oncol. 2011; 6:244–285.9. Rosado-de-Christenson ML, Templeton PA, Moran CA. Bronchogenic carcinoma: radiologic-pathologic correlation. Radiographics. 1994; 14:429–446. quiz 447-448
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Tripe synchronous primary lung cancer: one case report
- Synchronous Primary Lung Cancer with Differrent Squamous cell Carcinoma: One Case Report
- A case report of metachronous triple primary cancers including stomach, bladder and lung
- A Case of Primary Synchronous Lung Cancer
- Surgical Treatment for Multiple Primary Lung Cancer: Report of 2 cases
