Bone Cement-Augmented Percutaneous Short Segment Fixation: An Effective Treatment for Kummell's Disease?
- Affiliations
-
- 1Department of Natural Medical Sciences, College of Health Science, Chosun University, Gwangju, Korea.
- 2Department of Neurosurgery, Sun Han Hospital, Gwangju, Korea.
- 3Department of Thoracic and Cardiovascular Surgery, College of Medicine, Chosun University, Gwangju, Korea.
- 4Department of Neurosurgery, College of Medicine, Chosun University, Gwangju, Korea. chosunns@chosun.ac.kr
- KMID: 2067105
- DOI: http://doi.org/10.3340/jkns.2015.58.1.54
Abstract
OBJECTIVE
The aim of this prospective study was to evaluate the efficacy of bone cement-augmented percutaneous short segment fixation for treating Kummell's disease accompanied by severe osteoporosis.
METHODS
From 2009 to 2013, ten patients with single-level Kummell's disease accompanied by severe osteoporosis were enrolled in this study. After postural reduction for 1-2 days, bone cement-augmented percutaneous short segment fixation was performed at one level above, one level below, and at the collapsed vertebra. Clinical results, radiological parameters, and related complications were assessed preoperatively and at 1 month and 12 months after surgery.
RESULTS
Prior to surgery, the mean pain score on the visual analogue scale was 8.5+/-1.5. One month after the procedure, this score improved to 2.2+/-2.0 and the improvement was maintained at 12 months after surgery. The mean preoperative vertebral height loss was 48.2+/-10.5%, and the surgical procedure reduced this loss to 22.5+/-12.4%. In spite of some recurrent height loss, significant improvement was achieved at 12 months after surgery compared to preoperative values. The kyphotic angle improved significantly from 22.4+/-4.9degrees before the procedure to 10.1+/-3.8degrees after surgery and the improved angle was maintained at 12 months after surgery despite a slight correction loss. No patient sustained adjacent fractures after bone cement-augmented percutaneous short segment fixation during the follow-up period. Asymptomatic cement leakage into the paravertebral area was observed in one patient, but no major complications were seen.
CONCLUSION
Bone cement-augmented percutaneous short segment fixation can be an effective and safe procedure for Kummell's disease.
Keyword
Figure
-

Fig. 1 The component of intravertebral cleft is divided into gas and fluid. A : Intravertebral gas at L1 level is a computed tomographic finding indicative of Kummell's disease. B : Intravertebral fluid filled cleft at L1 level on magnetic resonance imaging is also characteristic of Kummell's disease.
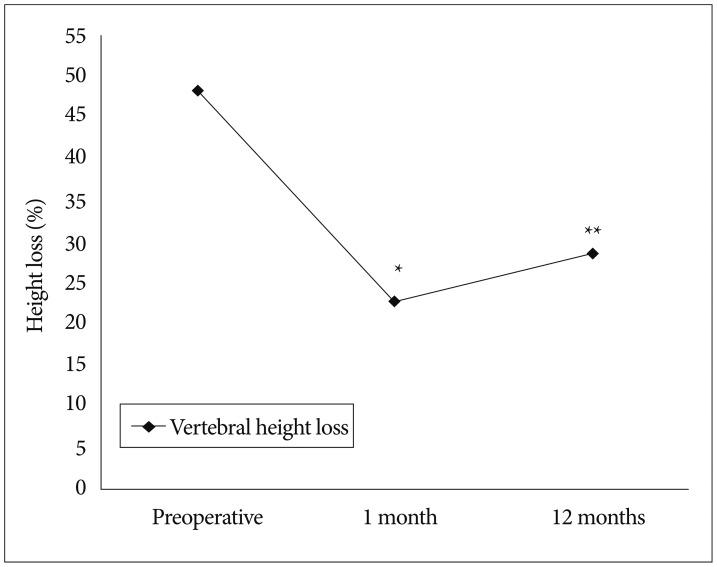
Fig. 2 Restoration of vertebral height. *Preoperative vs. 1 month, p=0.002, **Preoperative vs. 12 months, p=0.01.
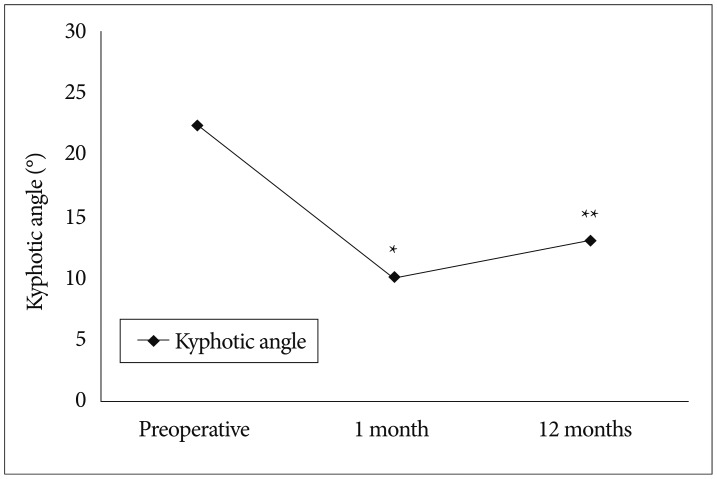
Fig. 3 Changes in kyphotic angle. *Preoperative vs. 1 month, p=0.005, **Preoperative vs. 12 months, p=0.018.

Fig. 4 Improvement in pain score. *p<0.001, preoperative vs. final follow-up. VAS : visual analogue scale.

Fig. 5 Osteoporotic compression fracture with an intravertebral cleft at the T12 level in a 85-year-old female. A : T2-weighted magnetic resonance image reveals a fluid filled IVC, indicative of Kummell's disease. B and C : Simple radiographs after bone cement-augmented percutneous short segment screw fixation show restored vertebral height and improved kyphotic deformity in spite of cement leakage through venous channel (arrow). D and E : Simple radiographs taken at 12 months after surgery show some aggravation of kyphosis.

Fig. 6 Osteoporotic compression fracture with an intravertebral cleft (IVC) at the L1 level in a 83-year-old male. A : Computed tomography scan shows a gas filled IVC, indicative of Kummell's disease. B and C : Simple radiographs after bone cement-augmented percutaneous short segment screw fixation show restored vertebral height and improved kyphotic deformity. D and E : Simple radiographs taken at 12 months after surgery reveal a well-maintained kyphotic angle.
Reference
-
1. Do HM, Jensen ME, Marx WF, Kallmes DF. Percutaneous vertebroplasty in vertebral osteonecrosis (Kummell's spondylitis). Neurosurg Focus. 1999; 7:e2. PMID: 16918233.2. Feng SW, Chang MC, Wu HT, Yu JK, Wang ST, Liu CL. Are intravertebral vacuum phenomena benign lesions? Eur Spine J. 2011; 20:1341–1348. PMID: 21533599.
Article3. Heo DH, Chin DK, Yoon YS, Kuh SU. Recollapse of previous vertebral compression fracture after percutaneous vertebroplasty. Osteoporos Int. 2009; 20:473–480. PMID: 18636218.
Article4. Jang JS, Kim DY, Lee SH. Efficacy of percutaneous vertebroplasty in the treatment of intravertebral pseudarthrosis associated with noninfected avascular necrosis of the vertebral body. Spine (Phila Pa 1976). 2003; 28:1588–1592. PMID: 12865850.
Article5. Kim HS, Kim SW, Ju CI, Lee SM, Shin H. Short segment fixation for thoracolumbar burst fracture accompanying osteopenia : a comparative study. J Korean Neurosurg Soc. 2013; 53:26–30. PMID: 23440679.
Article6. Kim KT, Suk KS, Kim JM, Lee SH. Delayed vertebral collapse with neurological deficits secondary to osteoporosis. Int Orthop. 2003; 27:65–69. PMID: 12700926.
Article7. Kummell H. Die rarefizierende ostitis der wirbelkrper. Deutsche Med. 1985; 21:180–181.8. Laredo JD. Expert's comment concerning Grand Rounds case entitled "Kümmell's disease : delayed post-traumatic osteonecrosis of the vertebral body" (by R. Ma, R. Chow, F. H. Shen). Eur Spine J. 2010; 19:1071–1072. PMID: 19937066.
Article9. Lee K, Lee SG, Kim WK, Yoo CJ, Park CW. Comparison vertebroplasty with kyphoplasty in delayed post-traumatic osteonecrosis of a vertebral body (Kummell's Disease). Korean J Spine. 2008; 5:70–76.10. Malghem J, Maldague B, Labaisse MA, Dooms G, Duprez T, Devogelaer JP, et al. Intravertebral vacuum cleft : changes in content after supine positioning. Radiology. 1993; 187:483–487. PMID: 8475295.
Article11. Saita K, Hoshino Y, Kikkawa I, Nakamura H. Posterior spinal shortening for paraplegia after vertebral collapse caused by osteoporosis. Spine (Phila Pa 1976). 2000; 25:2832–2835. PMID: 11064531.
Article12. Suk SI, Kim JH, Lee SM, Chung ER, Lee JH. Anterior-posterior surgery versus posterior closing wedge osteotomy in posttraumatic kyphosis with neurologic compromised osteoporotic fracture. Spine (Phila Pa 1976). 2003; 28:2170–2175. PMID: 14501932.
Article13. Wagner AL, Baskurt E. Refracture with cement extrusion following percutaneous vertebroplasty of a large interbody cleft. AJNR Am J Neuroradiol. 2006; 27:230–231. PMID: 16418390.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Short Segment Fixation for Thoracolumbar Burst Fracture Accompanying Osteopenia : A Comparative Study
- Bone Cement-Augmented Short Segment Fixation with Percutaneous Screws for Thoracolumbar Burst Fractures Accompanied by Severe Osteoporosis
- Kummell's Disease Managed by Percutaneous Vertebroplasty
- Delayed Bone Cement Displacement Following Balloon Kyphoplasty
- Posterior Screw Fixation in Previously Augmented Vertebrae with Bone Cement: Is It Inapplicable?
