Kummell's Disease Managed by Percutaneous Vertebroplasty
- Affiliations
-
- 1Department of Orthopedic Surgery, Ulsan University Hospital, University of Ulsan College of Medicine, Ulsan, Korea. yscho@uuh.ulsan.kr
- KMID: 2209739
- DOI: http://doi.org/10.4184/jkss.2001.8.3.226
Abstract
-
STUDY DESIGN: Prospective study about fourteen consecutive patients with Kummell's disease who were treated by percutaneous vertebroplasty with bone cement.
OBJECTIVES
To evaluate the results of percutaneous vertebroplasty using bone cement in the treatment of Kummell's disease. SUMMARY OF LITERATURE REVIEW: Kummell's disease is a rarely reported, poorly documented, and poorly understood phenomenon. It is associated with intravertebral vacuum phenomenon and clinically manifested by painful kyphosis. The treatment of the disease had been conservative or surgical reconstruction, but both conservative and operative treatment were not satisfactory in some patients.
MATERIALS AND METHODS
A review was conducted of 14 patients with 18 vertebrae treated with percutaneous vertebroplasty from June 1999 to May 2000. They had posttraumatic vertebral collapse or Kummell's disease and had failed medical therapy. Immediate and long-term pain response and complications of percutaneous vertebroplasty with bone cement were evaluated.
RESULTS
All patients reported complete relief of pain within the first 24 hours. Ten(71.5%) were evaluated as excellent; three(21.4%), good; one(7.1%), fair until 3 months postoperatively. Eight(57.2%) were evaluated as excellent; four(28.6%), good; fair(7.1%), one; poor(7.1%), one at final follow-up. Five(35.7%) patients had cement extrusion into the disc, paravertebral vessels and epidural space without significant systemic symptoms.
CONCLUSIONS
For patients with posttraumatic vertebral collapse or Kummell's disease, percutaneous vertebroplasty technique using bone cement would be a minimally invasive treatment option to achieve immediate relief of pain and stabilization without significant side effects.
MeSH Terms
Figure
-

Fig. 1. Initial AP and lateral radiographs (A) show no evidence of compression fracture, but the bone scan shows increased uptake on T12(B). Radiographs taken three months later show severe wedging of T12 and intravertebral gas shadow(C). After vertebroplasty, bone cement is well visualized in the T12 vertebral body with a leak into the T12-L1 disc space (D).
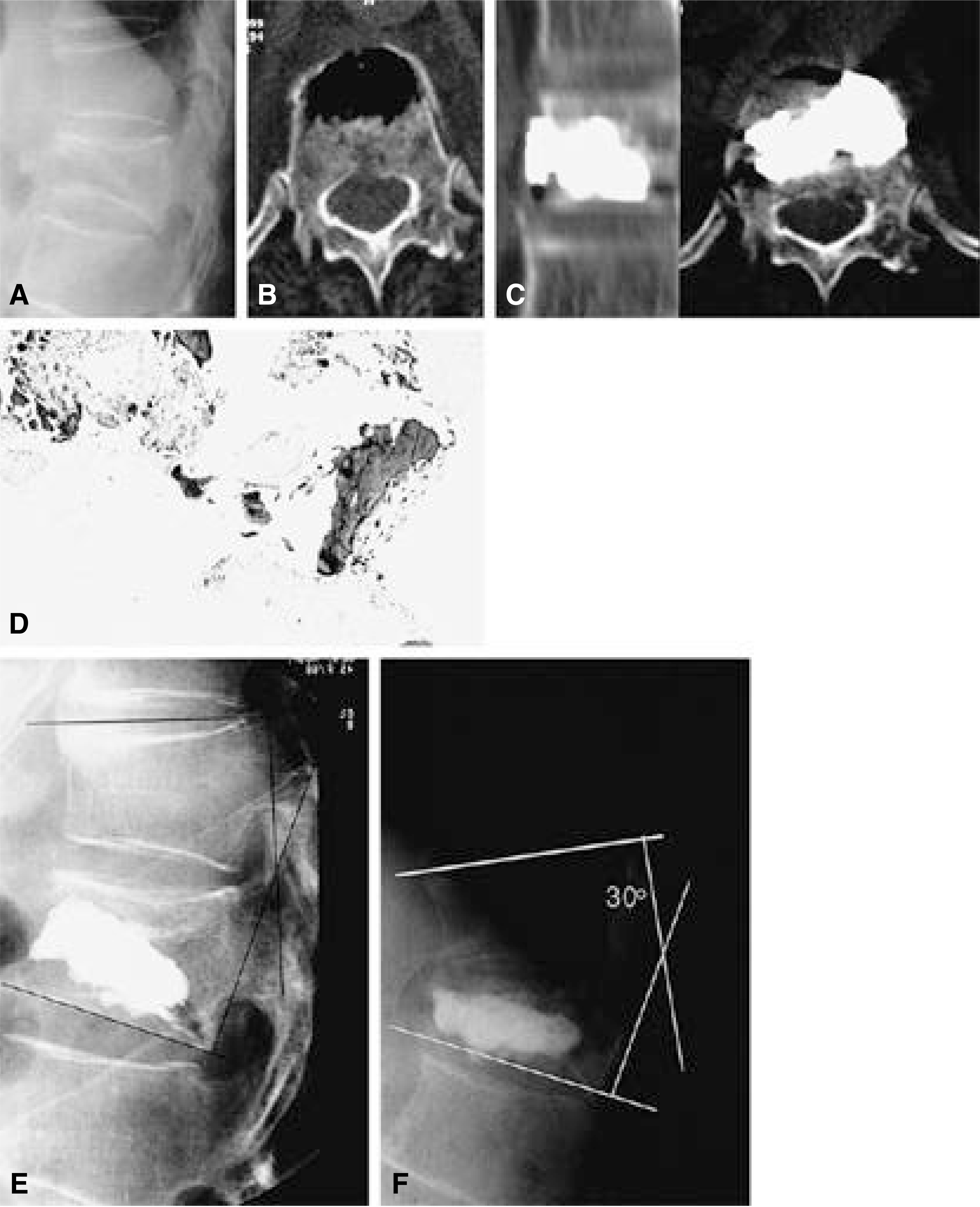
Fig. 2. Lateral radiograph (A) and CT (B) showing wedging of vertebral body and intravertebral gas. CT scans after vertebroplasty (C). Needle biopsy during vertebroplasty demonstrated ischemic necreosis of bone without evidence of bone regeneration (D). Kyphosis improved immediately vertebroplasty, but increased gradually after 2 years (E, F).
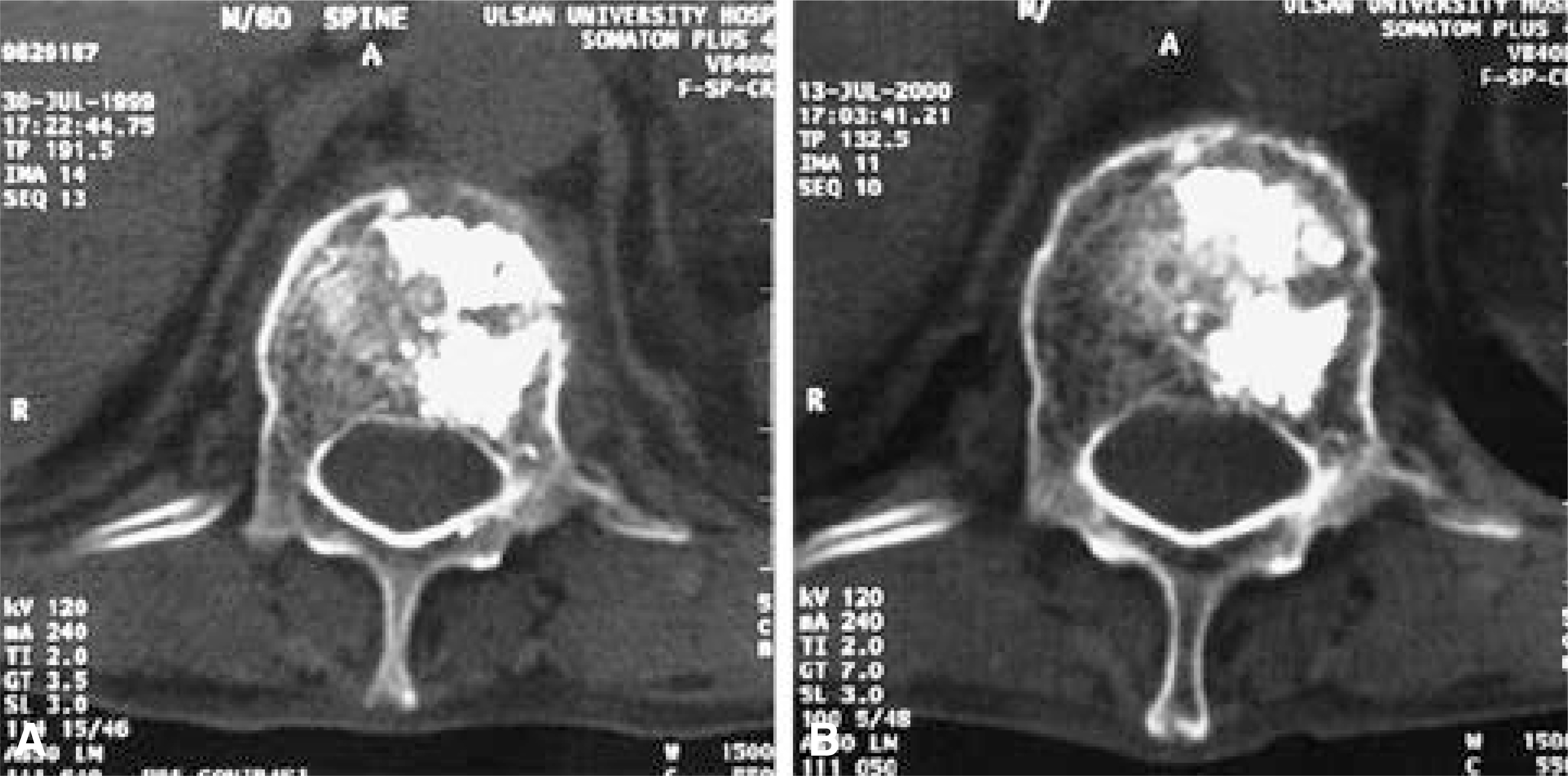
Fig. 3. CT scans taken immediately (A) and one year later (B) after vertebroplasty. The interface between bone and cement is well maintained without resoption of bone.
Cited by 2 articles
-
The Diagnosis of Osteoporotic Occult Vertebral Fracture and Vertebroplasty
Seong Jun Ahn, Bu Hwan Kim, Moo Ho Song, Seong Ho Yoo, Yeong Joon Kim
J Korean Fract Soc. 2012;25(3):208-214. doi: 10.12671/jkfs.2012.25.3.208.Clinical Results of Unilateral Partial Vertebroplasty(UPVP) in Osteoporotic Vertebral Fracture
Jun-Young Yang, June-Kyu Lee, Soo-Min Cha, Yong-Bum Joo
J Korean Soc Spine Surg. 2011;18(2):64-69. doi: 10.4184/jkss.2011.18.2.64.
Reference
-
1). Allen BL, Jinkins WJ. Vertebral osteonecrosis associated with pancreatitis in a child. J Bone Joint Surg. 60-A:985–987. 1985.2). Arciero RA, Leung KYK, Pierce JH. Spontaneous unstable burst fracture of the thoracolumbar spine in osteoporosis: A report of two cases. Spine. 14:114–117. 1989.3). Barr JD, Barr MS, Lemley TJ, McCann RM. Percutaneous vertebroplasty for pain relief and spinal stabilization, Spine. 25:923–928. 2000.4). Benedek TG, Nicholas JJ. Delayed traumatic vertebral body compression fracture part II: Pathologic features. Semin Arthritis Rheum. 23:653. 1980.
Article5). Benedek TG, Nicholas JJ, Reece JG. Kummell's Disease: A rare cause of posttraumatic back pain. Arthritis Rheum. 23:653. 1980.6). Bielecki DK, Sartoris D, Resnick D, Van Lom K, Fierer J, Haghighi P. Intraosseous and intradiscal gas in association with spinal infection: Report of three cases. American journal of Radiology. 147:83–86. 1986.
Article7). Brower AC, Downey EF Jr. Kummell's Disease: Report of a case with serial radiographs. Radiology. 141:363–364. 1981.8). Chevalier X, Wrona N, Avouac B, Larget-Piet B. Thigh pain and multiple vertebral osteonecrosis: Value of magnetic resonance imaging. J Rheumatol. 18:1627–1630. 1991.9). Chou LH, Knight RQ. Idiopathic avasular necrosis of a vertebral body: Case report and literature review. Spine. 22:1928–1932. 1997.10). Cotten A, Boutry N, Cortet B, et al. Percutaneous vertebroplasty: State of the art, Radiographics. 18:311–320. 1998.11). Deramond H, Depriester C, Galibert P, Le Gars D. Percutaneous vertebroplasty with polymethylmethacrylate. Technique, indications and results. Radiologic Clinics of North America. 36:533–546. 1998.12). Eenenaam DPV, EI-Khoury GY. Delayed post-traumatic vertebral collapse(Kummell's disease). Case report with serial radiographs, computed tomographic scans and bone scans. Spine. 18:1236–1241. 1993.13). Gagnerie F, Taillan B, Euller-Ziegler G. Inte rvertebral vacuum phenomenon in multiple myeloma. Clin Rheumatol. 6:579–599. 1987.14). Golimbu C, Firooznia H, Rafil M. The intravertebral vacuum sign. Spine. 11:1040–1042. 1985.
Article15). Ha KY, Kim KW, Park SJ, Paek DH, Ha JH. The surgical treatment of osteoporotic vertebral collapsecaused by minor trauma. J of Korean Orthop Assoc. 33:105–112. 1998.16). Ha KY, Moon MS, Lee NK, Chung CH. Kummell's disease -Report of three cases with serial radiographs-. J of Korean Society of Spine Surgery. 2:131–136. 1995.17). Hammererg KW, DeWald RL. Senile burst fracture: A complication of osteoporosis. Orthop Trans. 13:97. 1989.18). Hashimoto K, Yasui N, Yamagishi M, Kojimoto H, Mi-zuno K, Shimomura Y. Intravertebral vacuum cleft in the fifth lumbar vertebra. Spine. 14:351–354. 1989.
Article19). Hermann G, Goldblatt J, Desnick RJ. Kummell Disease: Delayed collapse of the traumatised spine in a patient with Gaucher type I disease. Br J Radiol. 57:833. 1984.20). Jaffe HL. Metabolic, Degenerative and Inflammatory Diseaase of Bones and Joints. Philadelphia: Lea and Febiger;pp621. 1972.21). Jensen ME, Evans AJ, Mathis JM, Kallmes DF, Cloft HJ, Dion JE. Percutaneous polymethylmethacrylate vertebroplasty in the treatment of osteoporotic vertebral body compression fracture: technical aspects. American Journal of Neuroradiology. 18:1897–1904. 1997.22). Kaemmerlen P, Thiesse P, Jonas P, et al. Percutaneous injection of orthopedic cement in metastatic vertebral lesions. N Engl J Med. 321:121. 1989.
Article23). Kaneda K, Ito M. Back pain and neurological deficits in osteoporotic spinal fractures. Hokkaido Journal of Medical Science. 72:381–387. 1997.24). Kempinsky WH. Osteoporotic kyphosis with paraplegia. Neurology. 8:181–186. 1958.
Article25). Kim YT, Lee CS, Noh KM, Paik DK, Cho YS, Kim CH. Surgical treatment for osteoporotic spine fractures. Korean Journal of Bone Metabolism. 6:141–152. 1999.26). Kumpan W, Salomonowitz E, Seidl G, Wittich GR. The intravertebral vacuum phenomenon. Skeletal Radiol. 15:444. 1986.
Article27). Larde D, Mathieu D, Frija J, Gaston A, Vasile N. Spinal vacuum phenomenon: CT diagnosis and significance. J Comput Assist Tomogr. 6:671. 1982.28). Lord CF, Herndon JH. Spinal cord compression secondary to kyphosis associated with radiation therapy for metastatic disease. Clin Orthop. 210:120–127. 1986.
Article29). Maldague BE, Noel HM, Malghem J. The intraver-tevral vacuum cleft: A sign of ischemic vertebral collapse. Radiology. 129:23–29. 1978.30). Nodena V, Maiocco I, Bosio C, Bianchi A, DeFilippi PG, Daneo V. Intravertebral vacuum cleft: Notes on five cases. Clinical and Experimental Radiology. 3:23–27. 1985.31). O'brien JP. Kyphosis secondary to infectious disease. Clin Orthop. 128:56–64. 1977.32). Resnick D, Niwayama G, Guerra J, Vint V, Ussel-man J. Spinal vacuum phenomena: Anatomical study and review. Radiology. 139:341–348. 1981.
Article33). Salomon C, Chopin D, Benoist M. Spinal cord compression: An exceptional complication of spinal osteoporosis. Spine. 13:222–224. 1988.34). Schabel SI, Moore TE, Rittenberg GM, Stanley JH, Leighton JH. Vertebral vacuum phenomenon. Skeletal Radiology. 4:154–156. 1979.
Article35). Schmorl G, Junghanns H. The Human Spine in Health and Disease. Second edition. New York: Grune and Stratton Compan;pp 167, 268-269. 1971.36). Shikata J, Yamamuro T, Iida H, Shimizu K, Yoshi-kawa J. Surgical treatment for paraplegia resulting from vertebral fractures in senile osteoporosis. Spine. 15:485–489. 1990.
Article37). Steel HH. Kummell's disease. American Journal of Surgery. 81:161–167. 1951.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Chronic Spinal Epidural Hematoma Related to Kummell's Disease
- One-stage multi-level vertebroplasty for a patient with a rapidly deteriorating condition due to multiple vertebral compression fractures: A case report
- Spontaneous Vertebral Reduction during the Procedure of Kyphoplasty in a Patient with Kummell's Disease
- More Effective Way to Perform Complete Percutaneous Vertebroplasty for Patients in Kummell’s Disease: A Case Report
- Vertebral Compression Fracture with Intravertebral Vacuum Cleft Sign: Pathogenesis, Image, and Surgical Intervention
