Atypical Pelvic Crescent Fracture Caused by Vertical Shear Force
- Affiliations
-
- 1Department of Orthopedic Surgery, The Catholic University of Korea, Daejeon St. Mary's Hospital, Daejeon, Korea. weonkim@hotmail.com
- KMID: 2054185
- DOI: http://doi.org/10.5371/hp.2014.26.3.194
Abstract
- The crescent fracture consists of a posterior iliac wing fracture with extension into the sacroiliac joint and a dislocation of the sacroiliac joint. This fracture represents a subset of lateral compression injury. The strong posterior ligaments of sacroiliac joint remain intact and a fracture fragment (crescent shape) involving the posterior superior iliac spines remains firmly attached to the sacrum. We report a patient with atypical pelvic crescent fracture that is mainly influenced by vertical shear injury and is characterized by posterior fracture-dislocations of the sacroiliac joint. In this case report, we review the literature on classification and treatment of atypical type of crescent fracture.
Figure
-

Fig. 1 Initial pelvis anteroposterior X-ray after injury of an 45-year-old patient with an AO/OTA type C1.2 with atypical pelvic crescent fracture that is mainly influenced by vertical shear injury and is characterized by posterior fracture-dislocations of the sacroiliac joint.
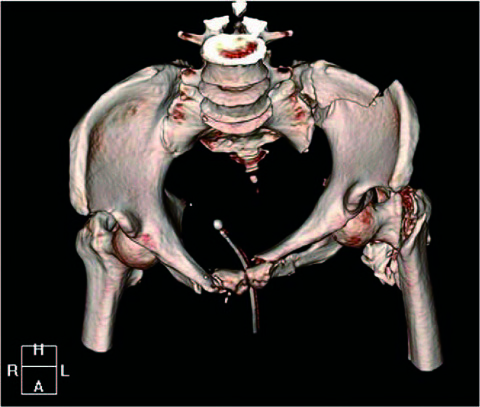
Fig. 2 Preoperative three dimensional computed tomography scan is helpful to figure out the configuration of pelvic ring injury.

Fig. 3 Pelvis anteroposterior X-ray 5 days after applying skeletal traction shows that the fractured site of posterior iliac wing was rarely reduced comparing with the initial X-ray.

Fig. 4 (A) Immediate postoperative radiographs of the patient shows well reduced state of sacroiliac joint, posterior iliac wing, symphysis pubis and intertrochanteric fracture of femur. (B) The last follow-up at postoperative 2 year and 6 month shows well maintained state.
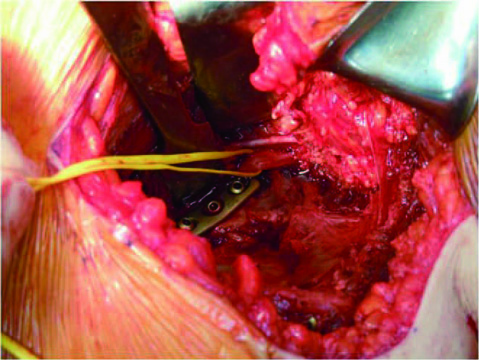
Fig. 5 Clinical photograph of the filth lumbar nerve root (surrounded by yellow vessel loop) which we found during surgery. We applied the plate and screws carefully not to irritate this nerve.
Reference
-
1. Day AC, Kinmont C, Bircher MD, Kumar S. Crescent fracture-dislocation of the sacroiliac joint: a functional classification. J Bone Joint Surg Br. 2007; 89:651–658.2. Oransky M, Tortora M. Nonunions and malunions after pelvic fractures: why they occur and what can be done? Injury. 2007; 38:489–496.
Article3. Thaunat M, Laude F, Paillard P, Saillant G, Catonné Y. Transcondylar traction as a closed reduction technique in vertically unstable pelvic ring disruption. Int Orthop. 2008; 32:7–12.
Article4. Borrelli J Jr, Koval KJ, Helfet DL. Operative stabilization of fracture dislocations of the sacroiliac joint. Clin Orthop Relat Res. 1996; 329:141–146.
Article5. Borrelli J Jr, Koval KJ, Helfet DL. The crescent fracture: a posterior fracture dislocation of the sacroiliac joint. J Orthop Trauma. 1996; 10:165–170.
Article6. Starr AJ, Walter JC, Harris RW, Reinert CM, Jones AL. Percutaneous screw fixation of fractures of the iliac wing and fracture-dislocations of the sacro-iliac joint (OTA Types 61-B2.2 and 61-B2.3, or Young-Burgess "lateral compression type II" pelvic fractures). J Orthop Trauma. 2002; 16:116–123.
Article7. Behrens F, Comfort T. Orthopaedic Trauma Association. Anterior fixation of dislocations and fracture-dislocations of the sacroiliac joint. In : Proceeding of OTA 2nd Annual Meeting; 1986 Nov 20-22; San Francisco, CA. San Francisco (CA): OTA;c1986.8. Matta JM. Indications for anterior fixation of pelvic fractures. Clin Orthop Relat Res. 1996; 329:88–96.
Article9. Templeman DC, Simpson T, Matta JM. Surgical management of pelvic ring injuries. Instr Course Lect. 2005; 54:395–400.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Intrapelvic Anterior Plate Fixation for Crescent Fracture-Dislocation of Sacroiliac Joint
- A Clinical Study of the Unstable Pelvic Fractures involving Sacro-iliac Joint
- Comparative finite element analysis of an osseointegration system in transradial amputation: a proposal of a new design for osseointegration
- The shear bond strength of two adhesives bonded to composite resin and glass ionomer cement restorations
- The Clinical Analysis of the Pelvic Fracture
