Intrapelvic Anterior Plate Fixation for Crescent Fracture-Dislocation of Sacroiliac Joint
- Affiliations
-
- 1Department of Orthopedic Surgery, Konkuk University Medical Center, Konkuk University School of Medicine, Seoul, Korea. damioh@gmail.com
- KMID: 1431662
- DOI: http://doi.org/10.12671/jkfs.2013.26.3.184
Abstract
- PURPOSE
To evaluate the radiological and clinical outcomes of intrapelvic anterior plate fixations for Day Classification Type II crescent fracture-dislocations of sacroiliac joints.
MATERIALS AND METHODS
Ten patients who had undertaken the surgical treatment for the sacroiliac joint from 2006 to 2012 were enrolled in this study. All cases fell into Type II by Day Classification for sacroiliac joint injuries. For surgical treatments, the plate fixation through the intra-pelvic anterior approach was first performed for all cases and anterior ring fixation was performed in 4 cases with more severely displaced anterior pelvic ring injuries. Then, radiological and clinical evaluation was implemented.
RESULTS
The bone union was observed from all patients whom performed the surgical fixation. In the radiological results, 9 cases with the anatomic and nearly-anatomic reductions were observed. Out of the 10 cases which performed the rotational displacement analysis, there were 3 excellent cases, 6 good cases and 1 fair case. The 10 cases that performed the deformity index and vertical displacement analysis, less variations were observed in the anterior ring fixations after intra-pelvic anterior plate fixation group. According to the clinical results, 4 excellent cases, 3 good cases, and 3 moderate cases were observed.
CONCLUSION
In the Type II crescent fracture-dislocation of sacroiliac joint, the intrapelvic anterior plate fixation achieved satisfactory anatomical reductions, radiological stabilities and clinical results.
Figure
-
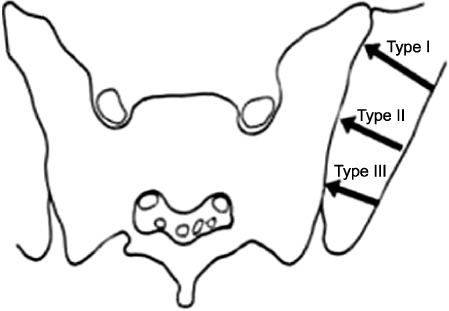
Fig. 1 Classification of crescent fractures according to Day et al. (Fig. 3D) with permission4).
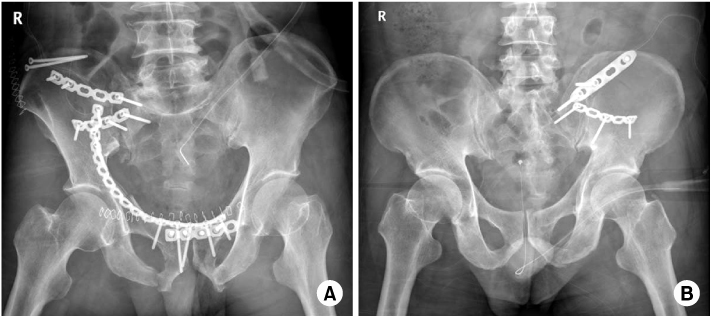
Fig. 2 (A) Radiograph shows intra-pelvic anterior approach & plate fixation with anterior ring fixation. (B) Radiograph shows intrapelvic anterior approach & plate fixation without anterior ring fixation.
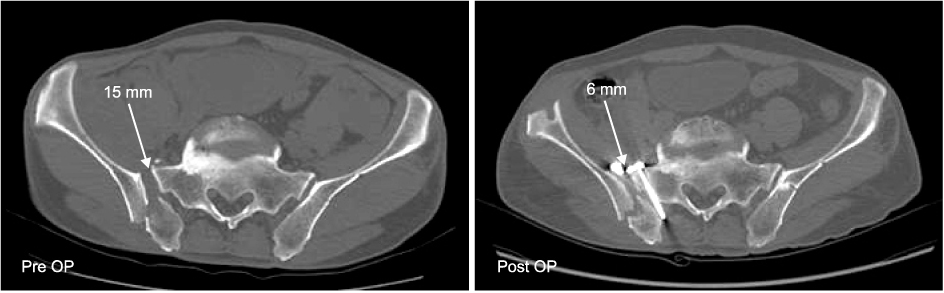
Fig. 3 Reduction of fracture-dislocation was evaluated with a comparison of pre- and post-operative computed tomography scans. Pre OP: Preoperative, Post OP: Postoperative.

Fig. 4 Rotational displacement was evaluated with a comparison of pre- and post-operative computed tomography scans. Pre OP: Preoperative, Post OP: Postoperative.
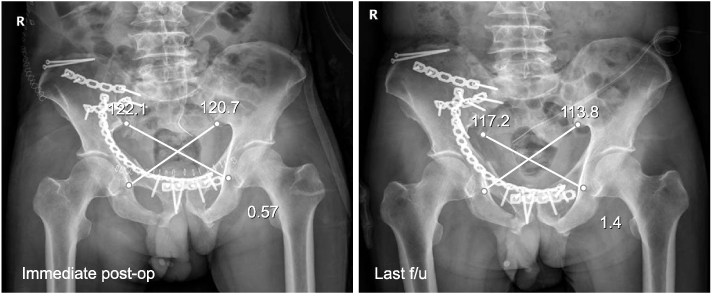
Fig. 5 Deformity index was evaluated with a comparison of immediate postoperative (post-op) and last follow-up (f/u) plain X-rays. Radiograph showing measurements of deformity index (X-Y/X+Y), which takes obliquity of the exposure into account, was the calculated (X-Y/X+Y).
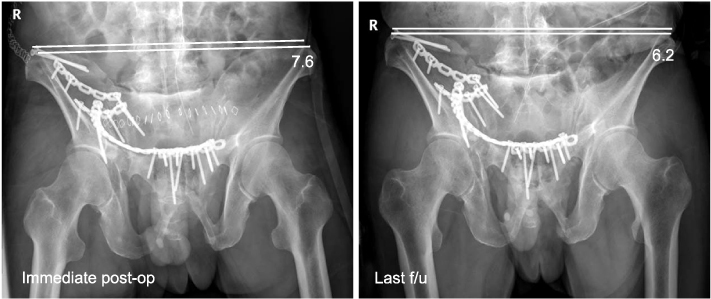
Fig. 6 Vertical displacement was evaluated with a comparison of immediate postoperative (postop) and recent follow-ups (f/u) of plain X-rays. Radiograph showing vertical displacement with the distance between the top of the iliac crests and a line perpendicular to the L5 reference line and the corrected displacement on the post-operative radiograph in the same patient.
Reference
-
1. Borrelli J Jr, Koval KJ, Helfet DL. Operative stabilization of fracture dislocations of the sacroiliac joint. Clin Orthop Relat Res. 1996; (329):141–146.
Article2. Borrelli J Jr, Koval KJ, Helfet DL. The crescent fracture: a posterior fracture dislocation of the sacroiliac joint. J Orthop Trauma. 1996; 10:165–170.
Article3. Burgess AR, Eastridge BJ, Young JW, et al. Pelvic ring disruptions: effective classification system and treatment protocols. J Trauma. 1990; 30:848–856.4. Day AC, Kinmont C, Bircher MD, Kumar S. Crescent fracture-dislocation of the sacroiliac joint: a functional classification. J Bone Joint Surg Br. 2007; 89:651–658.5. Helfet DL. Open reduction internal fixation of the pelvis. Tech Orthop. 1990; 4:67–78.
Article6. Holdsworth FW. Dislocation and fracture-dislocation of the pelvis. J Bone Joint Surg Br. 1948; 30B:461–466.
Article7. Kellam JF, McMurtry RY, Paley D, Tile M. The unstable pelvic fracture. Operative treatment. Orthop Clin North Am. 1987; 18:25–41.8. Keshishyan RA, Rozinov VM, Malakhov OA, et al. Pelvic polyfractures in children. Radiographic diagnosis and treatment. Clin Orthop Relat Res. 1995; (320):28–33.9. Lee JY, Moon DH, Kim GB. Prognosis of early internal fixation in unstable pelvic fractures. J Korean Soc Fract. 2000; 13:741–748.
Article10. Matta JM, Saucedo T. Internal fixation of pelvic ring fractures. Clin Orthop Relat Res. 1989; (242):83–97.
Article11. McCormack R, Strauss EJ, Alwattar BJ, Tejwani NC. Diagnosis and management of pelvic fractures. Bull NYU Hosp Jt Dis. 2010; 68:281–291.12. Pohlemann T, Bosch U, Gänsslen A, Tscherne H. The Hannover experience in management of pelvic fractures. Clin Orthop Relat Res. 1994; (305):69–80.
Article13. Ragnarsson B, Olerud C, Olerud S. Anterior square-plate fixation of sacroiliac disruption. 2-8 years follow-up of 23 consecutive cases. Acta Orthop Scand. 1993; 64:138–142.
Article14. Rommens PM, Hessmann MH. Staged reconstruction of pelvic ring disruption: differences in morbidity, mortality, radiologic results, and functional outcomes between B1, B2/B3, and C-type lesions. J Orthop Trauma. 2002; 16:92–98.
Article15. Routt ML Jr, Simonian PT, Mills WJ. Iliosacral screw fixation: early complications of the percutaneous technique. J Orthop Trauma. 1997; 11:584–589.
Article16. Shaw JA, Mino DE, Werner FW, Murray DG. Posterior stabilization of pelvic fractures by use of threaded compression rods Case reports and mechanical testing. Clin Orthop Relat Res. 1985; (192):240–254.17. Simpson LA, Waddell JP, Leighton RK, Kellam JF, Tile M. Anterior approach and stabilization of the disrupted sacroiliac joint. J Trauma. 1987; 27:1332–1339.
Article18. Starr AJ, Walter JC, Harris RW, Reinert CM, Jones AL. Percutaneous screw fixation of fractures of the iliac wing and fracture-dislocations of the sacro-iliac joint (OTA Types 61-B2.2 and 61-B2.3, or Young-Burgess "lateral compression type II" pelvic fractures). J Orthop Trauma. 2002; 16:116–123.
Article19. Tile M. Pelvic fractures: operative versus nonoperative treatment. Orthop Clin North Am. 1980; 11:423–464.
Article20. Young JW, Burgess AR, Brumback RJ, Poka A. Pelvic fractures: value of plain radiography in early assessment and management. Radiology. 1986; 160:445–451.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Atypical Pelvic Crescent Fracture Caused by Vertical Shear Force
- Plate Fixation for Sacroiliac Joint Separation Through the Anterior Approach
- Crescent Fracture-dislocation of Sacroiliac Joint: Affecting Factors of Operative Results
- Treatment of Traumatic Sternoclavicular Joint Anterior Dislocation with a Sternal Fracture
- Surgical Fixation of Sacroiliac Joint Complex in Unstable Pelvic Ring Injuries
