Hip Pelvis.
2013 Jun;25(2):121-126. 10.5371/hp.2013.25.2.121.
Recovery of Limitation of Motion in Secondary Osteoarthritis of the Hip Using Arthroscopy
- Affiliations
-
- 1Department of Orthopedic Surgery, Research Institute for Medical Science, Chungnam National University School of Medicine, Daejeon, Korea. dshwang@cnu.ac.kr
- 2On Orthopedic Clinic, Suwon, Korea.
- 3Department of Orthopaedic Surgery, Bumin Hospital, Busan, Korea.
- KMID: 2054149
- DOI: http://doi.org/10.5371/hp.2013.25.2.121
Abstract
- PURPOSE
To analyze the arthroscopic findings and treatment results of patients with a limitation of hip motion caused by early degenerative osteoarthritis.
MATERIALS AND METHODS
Retrospective analysis was performed on 13 patients who underwent arthroscopic treatment from May 2009 to March 2010, among patients with a limitation of hip motion and femoroacetabular impingement symptoms by early degenerative osteoarthritis. Head-neck offset, anteversion, and a change in the alpha angle was compared. At the final follow up, the VAS (Visual analogue scale), modified Harris hip score, and range of motion were compared.
RESULTS
The arthroscopic findings showed diffused synovitis in all 13 cases. Among them, 9 cases were accompanied with a labral tear, and 2 cases showed a labral deformity. The VAS decreased from 7.5 preoperatively to 1.8 postoperatively and the modified Harris hip score improved from 49.3(35-60) before surgery to 90.1(85-95) after surgery. Each flexion and internal rotation improved significantly (P<0.05) from 95.2degrees (60-120degrees) to 127.7degrees (110-140degrees) and 4.6degrees (-5-25degrees) to 25.4degrees (15-30degrees), respectively.
CONCLUSION
This study shows that the arthroscopic treatment of femoroacetabular impingement with a limitation of the range of motion by early degenerative arthritis can be expected with an improvement in flexion and internal rotation of the hip.
MeSH Terms
Figure
-
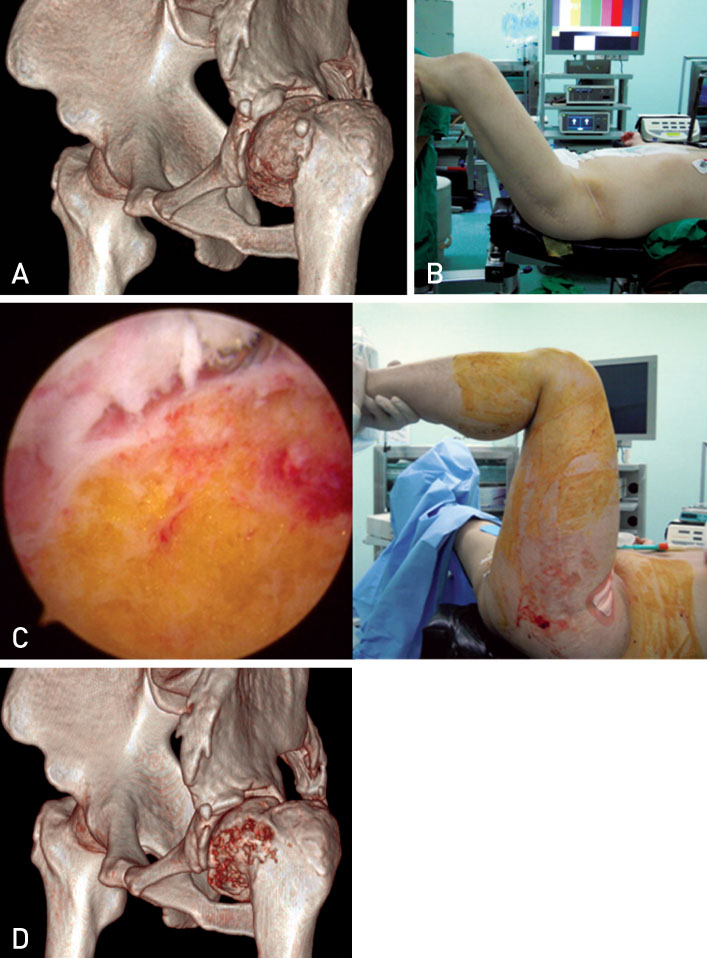
Fig. 1 32-year old male patient showed limitation of ROM due to sequelae of LCP of the left hip. (A) 3D CT image. (B) Preoperative measurement of flexion degree of the hip under general anesthesia. (C) Arthroscopic findings of the hip after performing femoroplasty, and flexion degree of the hip after operation. (D) Postoperative 3D CT findings.
Reference
-
1. Byrd JW, Jones KS. Adhesive capsulitis of the hip. Arthroscopy. 2006; 22:89–94.
Article2. Kelly BT, Weiland DE, Schenker ML, Philippon MJ. Arthroscopic labral repair in the hip: surgical technique and review of the literature. Arthroscopy. 2005; 21:1496–1504.
Article3. McCarthy JC. Hip arthroscopy: when it is and when it is not indicated. Instr Course Lect. 2004; 53:615–621.4. Sampson TG. Complications of hip arthroscopy. Clin Sports Med. 2001; 20:831–835.
Article5. Kim KW, Lee TH, Nam WD, Rhyu KH. Normal adult hip range of motion focusing hip flexion. J Korean Orthop Assoc. 2006; 41:361–367.
Article6. Philippon MJ, Christensen JC, Wahoff MS. Rehabilitation after arthroscopic repair of intra-articular disorders of the hip in a professional football athlete. J Sport Rehabil. 2009; 18:118–134.
Article7. Kubiak-Langer M, Tannast M, Murphy SB, Siebenrock KA, Langlotz F. Range of motion in anterior femoroacetabular impingement. Clin Orthop Relat Res. 2007; 458:117–124.
Article8. Eijer H, Myers SR, Ganz R. Anterior femoroacetabular impingement after femoral neck fractures. J Orthop Trauma. 2001; 15:475–481.
Article9. Siebenrock KA, Schoeniger R, Ganz R. Anterior femoroacetabular impingement due to acetabular retroversion. Treatment with periacetabular osteotomy. J Bone Joint Surg Am. 2003; 85:278–286.10. Torry MR, Schenker ML, Martin HD, Hogoboom D, Philippon MJ. Neuromuscular hip biomechanics and pathology in the athlete. Clin Sports Med. 2006; 25:179–197. vii
Article11. Ito H, Song Y, Lindsey DP, Safran MR, Giori NJ. The proximal hip joint capsule and the zona orbicularis contribute to hip joint stability in distraction. J Orthop Res. 2009; 27:989–995.
Article12. Shindle MK, Ranawat AS, Kelly BT. Diagnosis and management of traumatic and atraumatic hip instability in the athletic patient. Clin Sports Med. 2006; 25:309–326. ix–x.
Article13. Myers CA, Register BC, Lertwanich P, et al. Role of the acetabular labrum and the iliofemoral ligament in hip stability: an in vitro biplane fluoroscopy study. Am J Sports Med. 2011; 39:Suppl. 85S–91S.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Femoroacetabular Impingement Syndrome
- Clinical Application of Hip Arthroscopy in Degenerative Osteoarthritis
- Arthroscopic Adhesiolysis of Knee Ankylosis
- Comprehensive Review of Advancements in Hip Arthroscopy
- Midterm-clinical Outcomes after Hip Arthroscopy in Middle-aged Patients with Early Osteoarthritis
