Trans-sphenoidal Approach to the Supraclinoid Internal Carotid Artery for Endovascular Access in a Cadaver
- Affiliations
-
- 1Department of Neurological Surgery, Rush University Medical Center, Chicago, IL, USA. andrew_johnson@rush.edu
- 2Rush Medical College, Chicago, IL, USA.
- 3Department of Anatomy, Rush University Medical Center, Chicago, IL, USA.
- KMID: 2052078
- DOI: http://doi.org/10.5469/neuroint.2013.8.1.29
Abstract
- PURPOSE
Sometimes, intracranial pathology in the distal vasculature cannot be accessed by standard endovascular techniques because of occlusion or insurmountable tortuosity of theinternal carotid artery (ICA). A trans-sphenoidal surgical approach can follow a similar trajectory to the course of the supraclinoid ICA. This study evaluates the feasibility of a trans-sphenoidal approach to the supraclinoid ICA for endovascular access.
MATERIALS AND METHODS
In a fresh cadaver head, the sphenoid sinus was dissected through a trans-sphenoidal route. Bone over the carotid prominence was removed to expose the ICA. The artery was catheterized using the Seldinger technique, and three-dimensional digital subtraction angiography was performed to evaluate the procedure.
RESULTS
The catheter was successfully inserted into the supraclinoid ICA via the trans-sphenoidal route. Three-dimensional radiographic reconstruction confirmed placement of the catheter and the trajectory of the sheath into the supraclinoid ICA.
CONCLUSION
While the trans-sphenoidal route has innumerable disadvantages over the standard endovascular access techniques, this route could be considered when other treatment options are too risky or impractical.
MeSH Terms
Figure
-
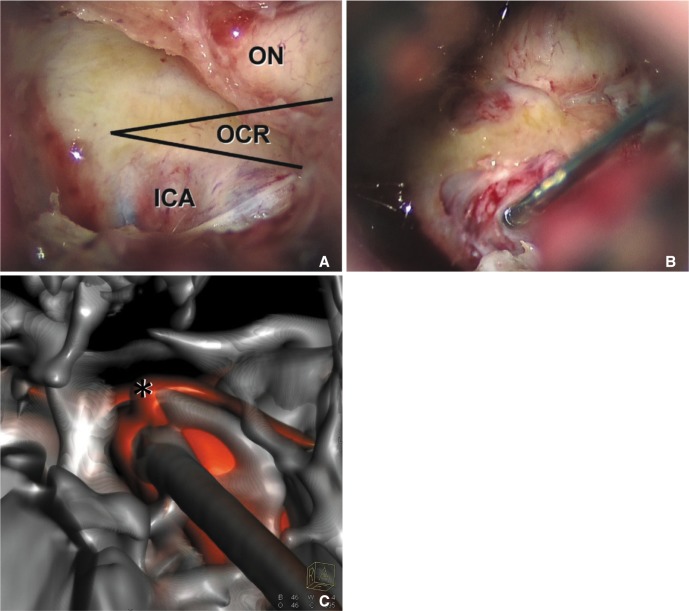
Fig. 1 (A) Microscopic view through the right naris into the left superolateral sphenoid sinus demonstrates the lateral opticocarotid recess (OCR) and bony prominences over the optic nerve (ON) and internal carotid artery (ICA), (B) wire access from the left naris into the left ICAprior to the cannulation with the access catheter, (C) dual volume three-dimensional reconstruction image of skull base and vessels shows the entrance of the catheter into the left supraclinoid ICA and the origin of ophthalmic artery (*), which was not visualized during dissection.

Fig. 2 Dual volume reconstruction images of skull base and vessels after contrast injection into the trans-sphenoidal catheter (A) sagittal embedded multiplanar reconstruction shows the trajectory of the catheter (black arrow) entering the left ICA (*) in its supraclinoid segment from the ipsilateral naris. (B) Access through the contralateral naris might improve axial trajectory (orange arrow).
Reference
-
1. Halbach VV, Higashida RT, Hieshima GB, Hardin CW. Direct puncture of the proximally occluded internal carotid artery for treatment of carotid cavernous fistulas. AJNR Am J Neuroradiol. 1989; 10:151–154. PMID: 2492715.2. Tsai YH, Weng HH, Chen YL, Wu YM, Wong HF. Treatment of recurrent carotid cavernous fistula by direct puncture of a previously trapped internal carotid artery. J Vasc Interv Radiol. 2010; 21:738–740. PMID: 20304678.
Article4. Kono Y, Prevedello DM, Snyderman CH, Gardner PA, Kassam AB, Carrau RL, et al. One thousand endoscopic skull base surgical procedures demystifying the infection potential: incidence and description of postoperative meningitis and brain abscesses. Infect Control Hosp Epidemiol. 2011; 32:77–83. PMID: 21121816.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Supraclinoid Internal Carotid Artery Fenestration Harboring an Unruptured Aneurysm and Another Remote Ruptured Aneurysm: Case Report and Review of the Literature
- Endovascular Treatment with a Stent-Graft for Internal Carotid Artery Laceration during Trans Sphenoidal Surgery: A Case Report
- Is the retrograde access for endovascular treatment of a traumatic carotid cavernous fistula associated with dissection of the ipsilateral carotid possible?
- Endovascular Treatment of Cavernous Sinus Dural Arteriovenous Fistula via Radial Artery and Median Cubital Vein
- Microsurgical Anatomy of the Supraclinoid Internal Carotid Artery
