Is the retrograde access for endovascular treatment of a traumatic carotid cavernous fistula associated with dissection of the ipsilateral carotid possible?
- Affiliations
-
- 1Department of Interventional Neuroradiology, Universidade Federal de São Paulo, São Paulo, SP, Brazil
- 2Department of Interventional Neuroradiology, Hospital Estadual Central, VitÓria ES, Brazil
- KMID: 2514339
- DOI: http://doi.org/10.7461/jcen.2021.E2020.05.002
Abstract
- This is a case demonstrating a combined traumatic lesion of the internal carotid artery (dissection and a carotid cavernous fistula [CCF]) in a patient who was beaten during a robbery and, while trying to escape, was hit by a vehicle. Endovascular approach for the treatment was chosen using the retrograde access from the vertebral artery to the cavernous sinus by posterior communicating (Pcom) artery due to the occlusion of the ipsilateral internal carotid. Because the artery access by the internal carotid was impossible, retrograde approach by vertebral artery and Pcom artery was done to treat the direct CCF. A patient presented with left hemiplegia and proptosis, chemosis, right eye ptosis. Computed tomography (CT) and CT angiography revealed a CCF of the right carotid. An arterial retrograde endovascular approach by the vertebral artery was used for CCF occlusion with coils. We present a rare case of a combined traumatic cerebrovascular lesion, right carotid artery dissection and a right direct CCF treated by a retrograde endovascular approach by the vertebral artery through the Pcom artery to reach the fistula point and achieved a complete cure of the CCF.
Keyword
Figure
-

Fig. 1. Right CCA DSA lateral view. (A) Early arterial phase of the right CCA. (B) Late arterial phase of the right CCA. CCA, common carotid artery; DSA, digital subtraction angiography.
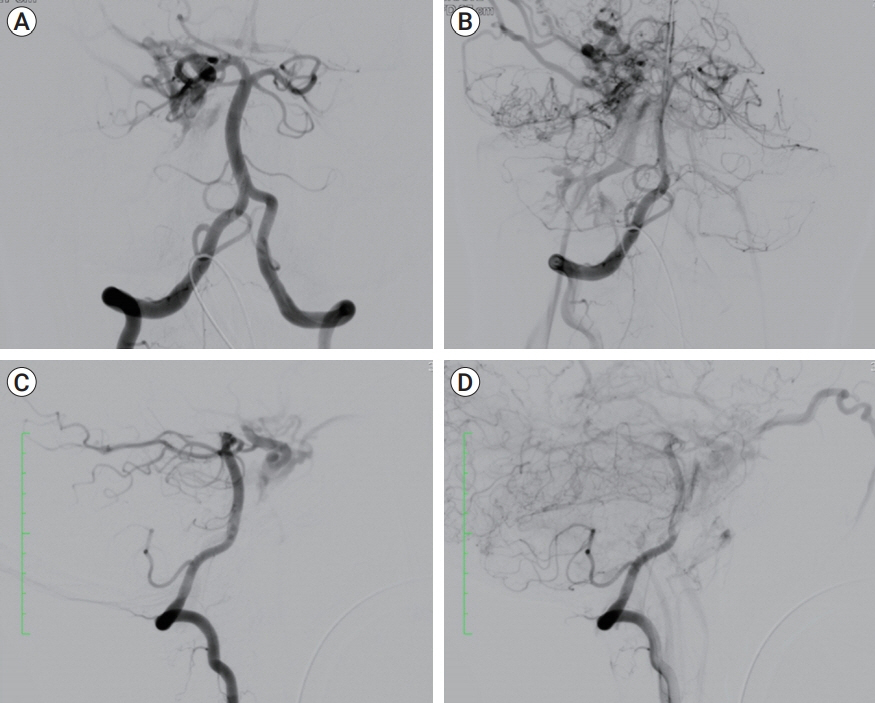
Fig. 2. Right vertebral artery DSA. (A) Early arterial phase (frontal view) before treatment. (B) Late arterial phase (frontal view) before treatment. (C) Early arterial phase (lateral view) before treatment. (D) Late arterial phase (lateral view) before treatment. DSA, digital subtraction angiography.

Fig. 3. Right vertebral artery DSA during the treatment. (A) Right vertebral artery roadmap (frontal view) with the microcatheter navigation throw the Pcom artery to achieve the fistular point. (B) Right vertebral artery DSA (lateral view) after microcatheter navigation. Highlighted with dotted line: Unsubtraction image with the microcatheter position. (C) First coil deployment. (D) Second coil deployment. (E, F) Positioned the microcatheter into the fistula point and Coils was detached to occlude the fistula point and the ICA beyond the ophthalmic artery. DSA, digital subtraction angiography; ICA, internal carotid artery.
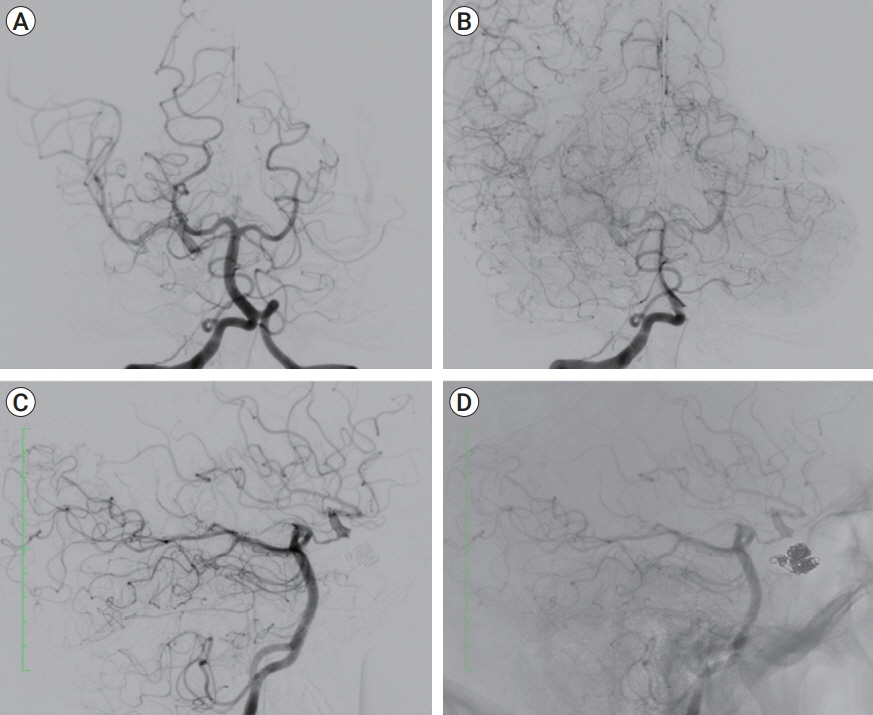
Fig. 4. Right vertebral artery DSA after treatment. (A) Early arterial phase of the right vertebral artery (frontal view) after endovascular treatment. (B) Late arterial phase of the right vertebral artery (frontal view) after endovascular treatment. (C) Early arterial phase (lateral view) after treatment. (D) Unsubtraction image of arterial phase (lateral view) after treatment. DSA, digital subtraction angiography.
Cited by 1 articles
-
Deconstructive repair of a direct carotid-cavernous fistula via a posterior circulation retrograde approach
Jonathan R. Crowe, Robert W. Regenhardt, Adam A. Dmytriw, Justin E. Vranic, Christopher J. Stapleton, Aman B. Patel
J Cerebrovasc Endovasc Neurosurg. 2024;26(4):394-398. doi: 10.7461/jcen.2024.E2023.05.001.
Reference
-
1. Barrow DL, Spector RH, Braun IF, Landman JA, Tindall SC, Tindall GT. Classification and treatment of spontaneous carotid-cavernous sinus fistulas. J Neurosurg. 1985; Feb. 62(2):248–56.
Article2. Biffl WL, Moore EE, Ryu RK, Offner PJ, Novak Z, Coldwell DM, et al. The unrecognized epidemic of blunt carotid arterial injuries: early diagnosis improves neurologic outcome. Ann Surg. 1998; Oct. 228(4):462–70.3. Chen CC, Chang PC, Shy CG, Chen WS, Hung HC. CT angiography and MR angiography in the evaluation of carotid cavernous sinus fistula prior to embolization: a comparison of techniques. AJNR Am J Neuroradiol. 2005; Oct. 26(9):2349–56.4. Debrun GM, Ausman JI, Charbel FT, Aletich VA. Access to the cavernous sinus through the vertebral artery: technical case report. Neurosurgery. 1995; Jul. 37(1):144–6. discussion 146-7.
Article5. De Campos JM, Ferro MO, Burzaco JA, Boixadós JR. Spontaneous carotid-cavernous fistula in osteogenesis imperfecta. J Neurosurg. 1982; Apr. 56(4):590–3.6. Ducruet AF, Albuquerque FC, Crowley RW, McDougall CG. The evolution of endovascular treatment of carotid cavernous fistulas: a single-center experience. World Neurosurg. 2013; Nov. 80(5):538–48.
Article7. Fox R, Pope FM, Narcisi P, Nicholls AC, Kendall BE, Hourihan MD, et al. Spontaneous carotid cavernous fistula in Ehlers Danlos syndrome. J Neurol Neurosurg Psychiatry. 1988; Jul. 51(7):984–6.
Article8. Gemmete JJ, Ansari SA, Gandhi D. Endovascular treatment of carotid cavernous fistulas. Neuroimaging Clin N Am. 2009; May. 19(2):241–55.
Article9. Halbach VV, Hieshima GB, Higashida RT, Reicher M. Carotid cavernous fistulae: indications for urgent treatment. AJR Am J Roentgenol. 1987; Sep. 149(3):587–93.
Article10. Higashida RT, Halbach VV, Tsai FY, Norman D, Pribram HF, Mehringer CM, et al. Interventional neurovascular treatment of traumatic carotid and vertebral artery lesions: results in 234 cases. AJR Am J Roentgenol. 1989; Sep. 153(3):577–82.
Article11. Lewis AI, Tomsick TA, Tew JM Jr. Management of 100 consecutive direct carotid- cavernous fistulas: Results of treatment with detachable balloons. Neurosurgery. 1995; Feb. 36(2):239–44. discussion 244-5.12. Meyers PM, Halbach VV, Dowd CF, Lempert TE, Malek AM, Phatouros CC, et al. Dural carotid cavernous fistula: definitive endovascular management and long-term follow-up. Am J Ophthalmol. 2002; Jul. 134(1):85–92.
Article13. Ohlsson M, Consoli A, Rodesch G. Endovascular treatment of carotico-cavernous fistulas with acrylic glue: a series of nine cases. Neuroradiology. 2016; Dec. 58(12):1181–8.
Article14. Posttraumatic intradural internal carotid artery-cavernous sinus fistula associated with ipsilateral carotid dissection. Transarterial embolization with detachable coils. Interv Neuroradiol. 2004; Mar. 10(1):63–8.15. Wilms G, Demaerel P, Lagae L, Casteels I, Mombaerts I. Direct caroticocavernous fistula and traumatic dissection of the ipsilateral internal carotid artery: endovascular treatment. Neuroradiology. 2000; Jan. 42(1):62–5.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Traumatic Carotid-cavernous Fistula Bringing about Intracerebral Hemorrhage
- Bilateral Traumatic Carotid-Cavernous Fistula
- A Case of Spontaneous of Traumatic Carotid Cavernous Fistula After Carotid Angiography
- Regional Cerebral Blood Flow Changes in Traumatic Carotid Cavernous Fistula During Trapping Procedure: Case Study, Preliminary Report
- A Case of the Carotid-Cavernous Fistula Due to the Internal Carotid Artery Injury During Endoscopic Sinus Surgery
