Transvenous Embolization of Cavernous and Paracavernous Dural Arteriovenous Fistula through the Facial Vein: Report of 12 Cases
- Affiliations
-
- 1Department of Neurosurgery, Seoul St. Mary's Hospital, The Catholic University of Korea, Seoul, Korea.
- 2Department of Radiology, St. Vincent's Hospital, The Catholic University of Korea, Suwon, Korea.
- 3Department of Radiology, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea.
- 4Department of Radiology, NHIC Ilsan Hospital of Korea, Ilsan, Korea.
- 5Department of Radiology, Seoul St. Mary's Hospital, The Catholic University of Korea, Seoul, Korea. bumrad@catholic.ac.kr
- KMID: 2052076
- DOI: http://doi.org/10.5469/neuroint.2013.8.1.15
Abstract
- PURPOSE
The aim of this study was to evaluate the feasibility and safety of the transfacial venous embolization of cavernous or paracavernous dural arteriovenous fistula (DAVF) in which approach via inferior petrosal sinus (IPS) was not feasible.
MATERIALS AND METHODS
We identified the cases of transfacial venous embolization of cavernous sinus (CS) or adjacent dural sinuses from the neurointerventional database of three hospitals. The causes and clinical and angiographic outcomes of transfacial venous embolization were retrospectively evaluated.
RESULTS
Twelve patients with CS (n = 11) or lesser wing of sphenoid sinus (LWSS, n = 1) DAVF were attempted to treat by transvenous embolization via ipsilateral (n = 10) or contralateral (n = 2) facial vein. Trans-IPS access to the target lesion was impossible due to chronic occlusion (n = 11) or acute angulation adjacent the target lesion (n = 1). In all twelve cases, it was possible to navigate through facial vein, angular vein, superior ophthalmic vein, and then CS. It was also possible to further navigation to contralateral CS through intercavernous sinus in two cases, and laterally into LWSS in one case. Post-treatment control angiography revealed complete occlusion of the DAVF in eleven cases and partial occlusion in one patient, resulting in complete resolution of presenting symptom in eight and gradually clinical improvement in four patients. There was no treatment-related complication during or after the procedure.
CONCLUSION
In the cavernous or paracavernous DAVF in which trans-IPS approach is not feasible, the facial vein seems to be safe and effective alternative route for transvenous embolization.
MeSH Terms
Figure
-

Fig. 1 Antero-posterior (A) and lateral (B) view of right ECA angiography show DAVF involving CS with arterial feeder from ECA and venous drainage to left SOV (large arrow), right sphenoparietal sinus and superficial middle cerebral vein through intercavernous sinus. (C, D) Through left facial vein (small arrows in figure A and B), the microwire was placed in right CS beyond the intercavernous sinus. (E) Coil embolization was performed for the shunt lesion using detachable and pushable fibered coils. (F) After the procedure, antero-posterior view of angiography selected right common carotid artery shows complete occlusion of the shunt.
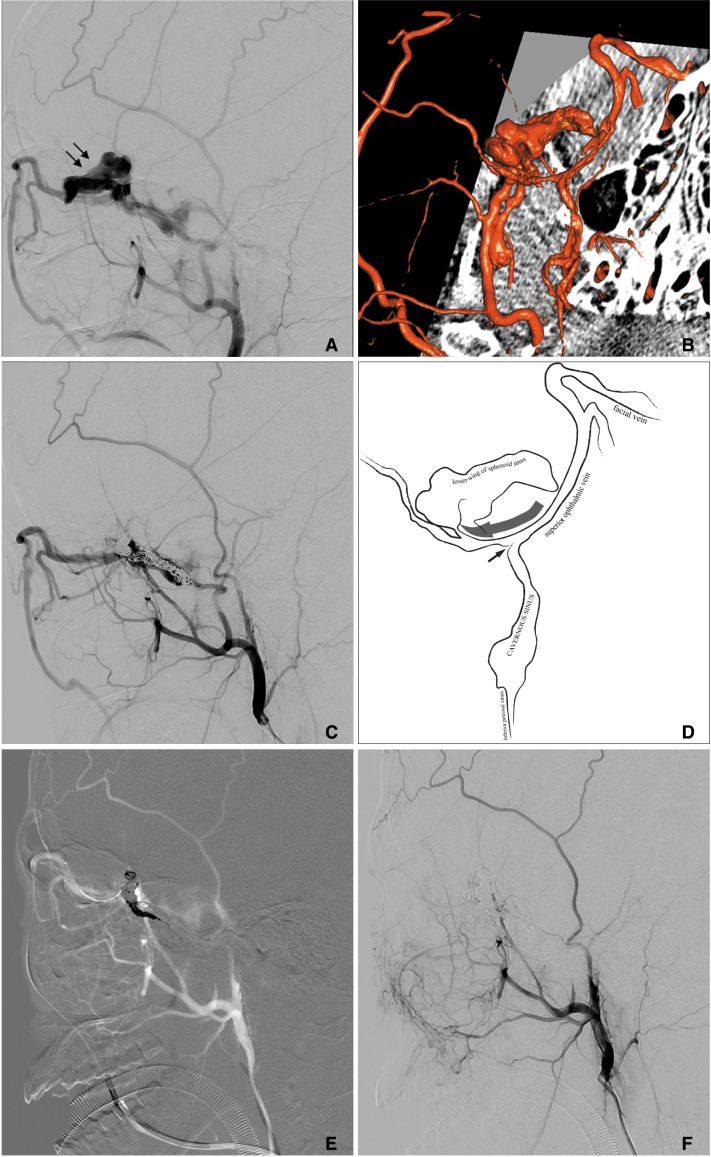
Fig. 2 Lateral view (A) and three-dimensional reconstruction image (B) of left ECA angiography showed DAVF with shunt flow into LWSS (arrows) connected with CS. The embolization for the lesion via arterial approach was performed using detachable and pushable fibered coils. (C) Follow-up angiography after 3 months showed recanalized shunt at the LWSS and venous drainage mainly into the SOV via the CS. The microcatheter was placed in the left IPS by microwire, and the left CS was selected. However, it could not be further advanced due to acute angle at the connection site (small arrow in figure D) between the LWSS and CS. (E) The microcatheter was placed in the left FV and SOV, and then it could be placed at the LWSS (through large arrow pathway in figure D). (F) The remnant shunt was complete occluded by coils.
Reference
-
1. Agid R, Willinsky RA, Haw C, Souza MP, Vanek IJ, terBrugge KG. Targeted compartmental embolization of cavernous sinus dural arteriovenous fistulae using transfemoral medial and lateral facial vein approaches. Neuroradiology. 2004; 46:156–160. PMID: 14655033.
Article2. Kim DJ, Kim DI, Suh SH, Kim J, Lee SK, Kim EY, et al. Results of transvenous embolization of cavernous dural arteriovenous fistula: a single-center experience with emphasis on complications and management. AJNR Am J Neuroradiol. 2006; 27:2078–2082. PMID: 17110671.3. Biondi A, Milea D, Cognard C, Ricciardi GK, Bonneville F, van Effenterre R. Cavernous sinus dural fistulae treated by transvenous approach through the facial vein: report of seven cases and review of the literature. AJNR Am J Neuroradiol. 2003; 24:1240–1246. PMID: 12812963.4. Benndorf G, Bender A, Lehmann R, Lanksch W. Transvenous occlusion of dural cavernous sinus fistulas through the thrombosed inferior petrosal sinus: report of four cases and review of the literature. Surg Neurol. 2000; 54:42–54. PMID: 11024506.
Article5. Elhammady MS, Peterson EC, Aziz-Sultan MA. Onyx embolization of a carotid cavernous fistula via direct transorbital puncture. J Neurosurg. 2011; 114:129–132. PMID: 20136392.
Article6. Quiñones D, Duckwiler G, Gobin PY, Goldberg RA, Viñuela F. Embolization of dural cavernous fistulas via superior ophthalmic vein approach. AJNR Am J Neuroradiol. 1997; 18:921–928. PMID: 9159371.7. Venturi C, Bracco S, Cerase A, Gennari P, Lorè F, Polito E, et al. Endovascular treatment of a cavernous sinus dural arteriovenous fistula by transvenous embolisation through the superior ophthalmic vein via cannulation of a frontal vein. Neuroradiology. 2003; 45:574–578. PMID: 12856091.
Article8. Oishi H, Arai H, Sato K, Iizuka Y. Complications associated with transvenous embolisation of cavernous dural arteriovenous fistula. Acta Neurochir (Wien). 1999; 141:1265–1271. PMID: 10672296.
Article9. Ha JG, Jeong HW, In HS, Choi SJ. Transvenous embolization of cavernous sinus dural arteriovenous fistula using the direct superior ophthalmic vein approach: a case report. Neurointervention. 2011; 6:100–103. PMID: 22125757.
Article10. Liu HM, Wang YH, Chen YF, Cheng JS, Yip PK, Tu YK. Long-term clinical outcome of spontaneous carotid cavernous sinus fistulae supplied by dural branches of the internal carotid artery. Neuroradiology. 2001; 43:1007–1014. PMID: 11760792.
Article11. Meyers PM, Halbach VV, Dowd CF, Lempert TE, Malek AM, Phatouros CC, et al. Dural carotid cavernous fistula: definitive endovascular management and long-term follow-up. Am J Ophthalmol. 2002; 134:85–92. PMID: 12095813.
Article12. Benndorf G, Bender A, Campi A, Menneking H, Lanksch WR. Treatment of a cavernous sinus dural arteriovenous fistula by deep orbital puncture of the superior ophthalmic vein. Neuroradiology. 2001; 43:499–502. PMID: 11465766.
Article13. Berlis A, Klisch J, Spetzger U, Faist M, Schumacher M. Carotid cavernous fistula: embolization via a bilateral superior ophthalmic vein approach. AJNR Am J Neuroradiol. 2002; 23:1736–1738. PMID: 12427633.14. Derang J, Ying H, Long Y, Reifa S, Qiming W, Yimu F, et al. Treatment of carotid-cavernous sinus fistulas retrograde via the superior ophthalmic vein (SOV). Surg Neurol. 1999; 52:286–292. PMID: 10511088.
Article15. Courtheoux P, Huet H, Tournade A, Theron J. Dural fistula of the cavernous sinus. Treatment through an intravenous approach apropos of 4 cases. J Neuroradiol. 1995; 22:301–308. PMID: 8636805.16. Dashti SR, Fiorella D, Spetzler RF, Albuquerque FC, McDougall CG. Transorbital endovascular embolization of dural carotid-cavernous fistula: access to cavernous sinus through direct puncture: case examples and technical report. Neurosurgery. 2011; 68:75–83. PMID: 21304335.
Article17. Goldberg RA, Goldey SH, Duckwiler G, Vinuela F. Management of cavernous sinus-dural fistulas. Indications and techniques for primary embolization via the superior ophthalmic vein. Arch Ophthalmol. 1996; 114:707–714. PMID: 8639083.18. Yu SC, Cheng KM, Tam PH, Wong GK, Chan CM, Cheung YL, et al. A venographic operational classification for transvenous embolization of dural carotid-cavernous fistula. Neuroradiology. 2011; 53:993–999. PMID: 21181141.
Article19. San Millan Ruiz D, Fasel JH, Rufenacht DA, Gailloud P. The sphenoparietal sinus of breschet: does it exist? An anatomic study. AJNR Am J Neuroradiol. 2004; 25:112–120. PMID: 14729539.20. Bitoh S, Arita N, Fujiwara M, Ozaki K, Nakao Y. Dural arteriovenous malformation near the left sphenoparietal sinus. Surg Neurol. 1980; 13:345–349. PMID: 7384999.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Transvenous Embolization of Cavernous Sinus Dural Arteriovenous Fistula Using the Direct Superior Ophthalmic Vein Approach: A Case Report
- Facilitated Retrograde Access via the Facial Vein for Transvenous Embolization of the Cavernous Sinus Dural Arteriovenous Fistula with Isolated Ophthalmic Venous Drainage
- Transvenous Coil Embolization for Dural Arteriovenous Fistulas of the Ophthalmic Sheath: Report of Two Cases and Review of the Literature
- Transvenous Embolization of Dural Carotid Cavernous Fistula through the Supraorbital Vein
- Transvenous injection of n-butyl 2-cyanoacrylate to obliterate the pathologic cavernous sinus as a salvage technique for incompletely obliterated complex cavernous sinus dural arteriovenous fistula after transvenous coil embolization
