Obstet Gynecol Sci.
2014 Sep;57(5):412-414. 10.5468/ogs.2014.57.5.412.
Mesenteric desmoid-type fibromatosis causing secondary hypertension in a young woman
- Affiliations
-
- 1Department of Obstetrics and Gynecology, Seoul Paik Hospital, Inje University College of Medicine, Seoul, Korea. tttnii@paik.ac.kr
- KMID: 2051726
- DOI: http://doi.org/10.5468/ogs.2014.57.5.412
Abstract
- This report describes an 18-year-old woman presenting with abdominal distension, left flank pain, and hypertension. She had a huge abdominal mass, diagnosed as a mesenteric desmoid-type fibromatosis, causing compression of the left external iliac vessels and ureter, as well as elevated renin concentration and hypertension. After surgical removal of the mass, all signs improved including hypertension.
MeSH Terms
Figure
-
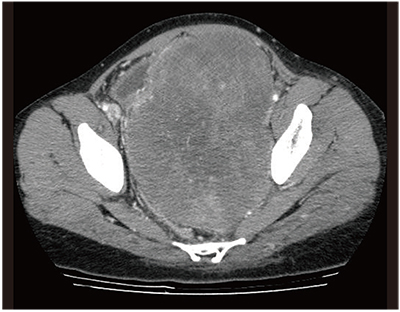
Fig. 1 Abdominal computed tomography, showing a huge lobulated mass with heterogeneous attenuation.
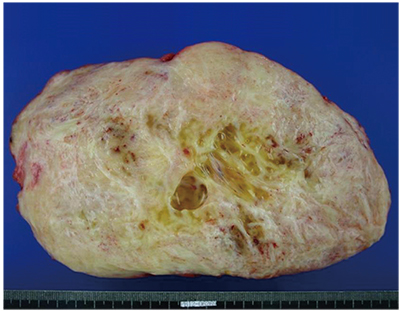
Fig. 2 Cut section with homogeneous appearance and multifocal petechial hemorrhaging.
Reference
-
1. Goldblum JR, Fletcher JA. Desmoid-type fibromatoses. In : Fletcher CD, Unni KK, Mertens F, editors. Pathology and genetics of tumors of soft tissue and bone. Lyon: IARC Press;2002. p. 83–84.2. Enzinger FM, Weiss SW. Fibromatoses. In : Enzinger FM, Weiss SW, editors. Soft tissue tumors. 3rd ed. St Louis: Mosby;1995. p. 201–229.3. Federle MP. Diagnostic imaging: abdomen. 1st ed. Salt Lake City: Amirsys;2004. p. 54–57.4. Naylor EW, Gardner EJ, Richards RC. Desmoid tumors and mesenteric fibromatosis in Gardner's syndrome: report of kindred 109. Arch Surg. 1979; 114:1181–1185.5. Simon NL, Mazur MT, Shingleton HM. Pelvic fibromatosis: an unusual gynecologic tumor. Obstet Gynecol. 1985; 65:767–769.6. Brooks AP, Reznek RH, Nugent K, Farmer KC, Thomson JP, Phillips RK. CT appearances of desmoid tumours in familial adenomatous polyposis: further observations. Clin Radiol. 1994; 49:601–607.7. Clark SK, Smith TG, Katz DE, Reznek RH, Phillips RK. Identification and progression of a desmoid precursor lesion in patients with familial adenomatous polyposis. Br J Surg. 1998; 85:970–973.8. Einstein DM, Tagliabue JR, Desai RK. Abdominal desmoids: CT findings in 25 patients. AJR Am J Roentgenol. 1991; 157:275–279.9. Chen YJ, Tam KW, Chen CS, Wu CH, Chen SC, Chan WP, et al. Case report: spontaneous isolated mesenteric fibromatosis presenting as megaduodenum. J Gastroenterol Hepatol. 1998; 13:383–386.10. Messiou C, Chalmers AG, Dexter S. An unusual case of ureteric obstruction. Br J Radiol. 2005; 78:848–850.11. Smith AJ, Lewis JJ, Merchant NB, Leung DH, Woodruff JM, Brennan MF. Surgical management of intra-abdominal desmoid tumours. Br J Surg. 2000; 87:608–613.12. Baliski CR, Temple WJ, Arthur K, Schachar NS. Desmoid tumors: a novel approach for local control. J Surg Oncol. 2002; 80:96–99.13. Hansmann A, Adolph C, Vogel T, Unger A, Moeslein G. High-dose tamoxifen and sulindac as first-line treatment for desmoid tumors. Cancer. 2004; 100:612–620.14. Klemi P, Alanen K, Hietanen S, Grenman S, Varpula M, Salmi T. Response of estrogen receptor-positive intraabdominal fibromatosis to aromatase inhibitor therapy. Obstet Gynecol. 2003; 102(5 Pt 2):1155–1158.
