Congenital Internal Hernia Presented with Life Threatening Extensive Small Bowel Strangulation
- Affiliations
-
- 1Department of Pediatrics, Pusan National University Yangsan Hospital, Yangsan, Korea. moonmissing@gmail.com
- 2Department of Surgery, Pusan National University Yangsan Hospital, Yangsan, Korea.
- 3Department of Radiology, Pusan National University Yangsan Hospital, Yangsan, Korea.
- KMID: 2051333
- DOI: http://doi.org/10.5223/pghn.2013.16.3.190
Abstract
- Internal hernia (IH) is a rare cause of small bowel obstruction occurs when there is protrusion of an internal organ into a retroperitoneal fossa or a foramen in the abdominal cavity. IH can be presented with acute or chronic abdominal symptom and discovered by accident in operation field. However, various kinds of imaging modalities often do not provide the assistance to diagnose IH preoperatively, but computed tomography (CT) scan has a high diagnostic accuracy. We report a case of congenital IH in a 6-year-old boy who experienced life threatening shock. CT scan showed large amount of ascites, bowel wall thickening with poor or absent enhancement of the strangulated bowel segment. Surgical exploration was performed immediately and had to undergo over two meters excision of strangulated small bowel. To prevent the delay in the diagnosis of IH, we should early use of the CT scan and take urgent operation.
Keyword
Figure
-
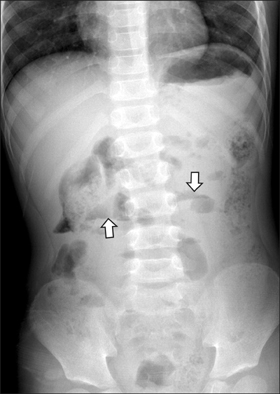
Fig. 1 Initial erect abdominal plain radiograph shows several irregular small bowel air without definite small bowel dilatation. Note two bowel loops with air-fluid level (arrows). These findings are abnormal but not specific.
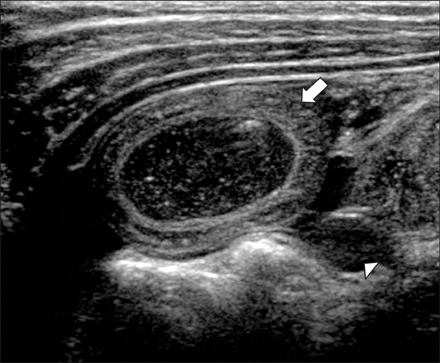
Fig. 2 Initial ultrasonography of the abdomen shows concentric wall thickening of the distended small bowel loop (arrow). Note the ascites (arrowhead).
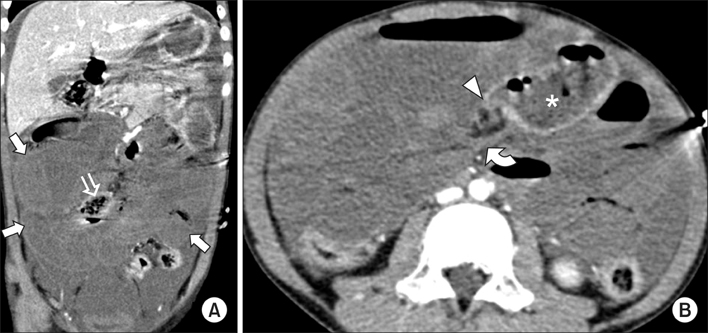
Fig. 3 Contrast-enhanced computed tomography (CT) scan of the abdomen and pelvis. (A) Coronal reformatted image shows large amount of ascites and extensive involvement of wall thickening and absent enhancement of the small bowel that indicate strangulation (arrows). Note the upward course of the terminal ileum (open arrow). (B) Axial CT scan demonstrated beaklike narrowing at the transition zone (arrowhead: serrated beak sign) and whirl of the obstructed bowel (curved arrow: whirl sign) which may suggest closed loop obstruction. Note the feculent matter mingled with gas bubbles within the lumen of dilated small bowel segment (asterisk: small bowel feces sign).

Fig. 4 Intraoperative photograph revealed herniating gangrenous bowel through small bowel mesenteric defect in operation field.
Reference
-
1. Cazejust J, Lafont C, Raynal M, Azizi L, Tourabi AC, Menu Y. Internal hernia through the omental foramen. Answer to the e-quid "Epigastric pain with sudden onset". Diagn Interv Imaging. 2013; 94:663–666.
Article2. Jain SK, Kaza RC, Garg PK. Incidental congenital transmesenteric hernia in an adult. Eur Rev Med Pharmacol Sci. 2011; 15:461–462.3. Tang V, Daneman A, Navarro OM, Miller SF, Gerstle JT. Internal hernias in children: spectrum of clinical and imaging findings. Pediatr Radiol. 2011; 41:1559–1568.
Article4. Zissin R, Hertz M, Gayer G, Paran H, Osadchy A. Congenital internal hernia as a cause of small bowel obstruction: CT findings in 11 adult patients. Br J Radiol. 2005; 78:796–802.
Article5. Butterworth J, Cross T, Butterworth W, Mousa P, Thomas S. Transmesenteric hernia: a rare cause of bowel ischaemia in adults. Int J Surg Case Rep. 2013; 4:568–570.
Article6. Kakimoto Y, Abiru H, Kotani H, Ozeki M, Tsuruyama T, Tamaki K. Transmesenteric hernia due to double-loop formation in the small intestine: a fatal case involving a toddler. Forensic Sci Int. 2012; 214:e39–e42.
Article7. Boudiaf M, Soyer P, Terem C, Pelage JP, Maissiat E, Rymer R. CT evaluation of small bowel obstruction. Radiographics. 2001; 21:613–624.
Article8. Kim JS, Chung JY, Park DC, Kim SW, Kim HJ, Kim YH. A case of intestinal malrotation with midgut volvulus presenting with intermittent vomiting and abdominal pain. Korean J Pediatr Gastroenterol Nutr. 2002; 5:79–82.
Article9. Bass KN, Jones B, Bulkley GB. Current management of small-bowel obstruction. Adv Surg. 1997; 31:1–34.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Laparoscopic double mesh repair of a large Morgagni hernia: a video vignette
- A Transmesenteric Hernia in a Child: Gangrene of a Long Segment of Small Bowel through a Large Mesenteric Defect
- Paraesophageal Hernia with Small Bowel Strangulation
- A Case of Small Bowel Obstruction Due to a Paracecal Hernia
- A Parastomal Hernia Causing Small Bowel Obstruction
