Tuberc Respir Dis.
2010 Feb;68(2):93-96. 10.4046/trd.2010.68.2.93.
A Case of Papillary Adenocarcinoma Presenting with Multiple Cysts
- Affiliations
-
- 1Department of Internal Medicine, Gil Medical Center, Gachon University of Medicine and Science, Incheon, Korea. light@gilhospital.com
- 2Department of Radiology, Gil Medical Center, Gachon University of Medicine and Science, Incheon, Korea.
- 3Department of Pathology, Gil Medical Center, Gachon University of Medicine and Science, Incheon, Korea.
- KMID: 2050591
- DOI: http://doi.org/10.4046/trd.2010.68.2.93
Abstract
- A 23-year old woman was admitted to our hospital with hemoptysis. The chest X-ray showed reticulonodular opacity and multiple cysts throughout the entire lung field. The chest CT scan revealed numerous bilateral cysts with various sizes, some of them with thickened walls. An open lung wedge resection was performed. The resected specimen showed scattered small nodules, 0.3 to 0.6 cm in size. Microscopically, each nodule was composed of atypical glands with an occasional papillary architecture spreading to the alveolar septa, which were morphologically consistent with a papillary adenocarcinoma with a bronchioloalveolar carcinoma growth pattern. Immunochemically, the tumor cells were negative for the S-100 protein. The patient was diagnosed with an adenocarcinoma of the lung. A variety of diseases can produce or mimic multiple, thin-walled cysts in the lung. Lung cancer with multiple cysts is quite rare. Nevertheless, adenocarcinoma should be a diagnostic consideration. We report a case of a multiple cystic adenocarcinoma of the lung.
Keyword
MeSH Terms
Figure
-
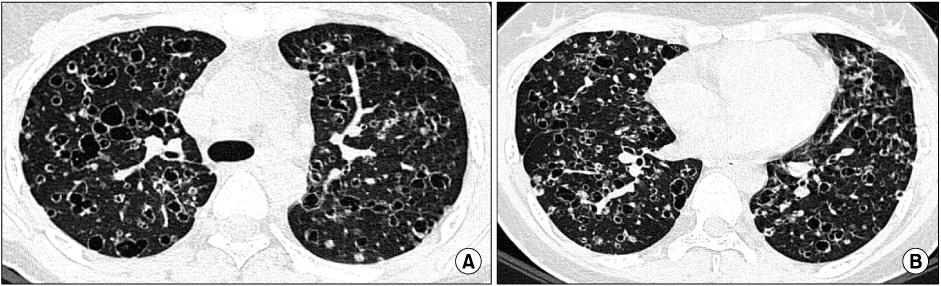
Figure 1 High-resolution CT images at the level of the carina (A) and right inferior pulmonary vein (B) reveal numerous bilateral cysts of various size, some of them with thickened walls.

Figure 2 (A) Histological examination shows scattered small nodules (arrows) (H&E stain, ×100). (B) In high power field view, tumor shows proliferation of papillary adenocarcinoma with lepidic growth pattern (H&E stain, ×400).

Figure 3 After 4th cycle chemotherapy, volumetric CT images at the level of the carina (A) and right inferior pulmonary vein (B) demonstrate multiple thin-walled cysts that are enlarged in the interim.
Reference
-
1. Hansell DM, Bankier AA, MacMahon H, McLoud TC, Müller NL, Remy J. Fleischner society: glossary of terms for thoracic imaging. Radiology. 2008. 246:697–722.2. Woodring JH, Fried AM. Significance of wall thickness in solitary cavities of the lung: a follow-up study. AJR Am J Roentgenol. 1983. 140:473–474.3. Woodring JH. Unusual radiographic manifestations of lung cancer. Radiol Clin North Am. 1990. 28:599–618.4. Chaudhuri MR. Primary pulmonary cavitating carcinomas. Thorax. 1973. 28:354–366.5. Woodring JH, Stelling CB. Adenocarcinoma of the lung: a tumor with a changing pleomorphic character. AJR Am J Roentgenol. 1983. 140:657–664.6. Hill CA. Bronchioloalveolar carcinoma: a review. Radiology. 1984. 150:15–20.7. Dodd GD, Boyle JJ. Excavating pulmonary metastases. Am J Roentgenol Radium Ther Nucl Med. 1961. 85:277–293.8. Ohba S, Takashima T, Hamada S, Kitagawa M. Multiple cystic cavitary alveolar-cell carcinoma. Radiology. 1972. 104:65–66.9. Weisbrod GL, Towers MJ, Chamberlain DW, Herman SJ, Matzinger FR. Thin-walled cystic lesions in bronchioalveolar carcinoma. Radiology. 1992. 185:401–405.10. Ryu JH, Swensen SJ. Cystic and cavitary lung diseases: focal and diffuse. Mayo Clin Proc. 2003. 78:744–752.11. Grant LA, Babar J, Griffin N. Cysts, cavities, and honeycombing in multisystem disorders: differential diagnosis and findings on thin-section CT. Clin Radiol. 2009. 64:439–448.12. Godwin JD, Webb WR, Savoca CJ, Gamsu G, Goodman PC. Multiple, thin-walled cystic lesions of the lung. AJR Am J Roentgenol. 1980. 135:593–604.13. Mahadeva R, Stewart S, Wallwork J. Metastatic endometrial stromal sarcoma masquerading as pulmonary lymphangioleiomyomatosis. J Clin Pathol. 1999. 52:147–148.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Multiple Papillary Adenocarcinoma of the Extrahepatic Bile Duct : Findings of ERCP
- Papillary gastric adenocarcinoma
- Invasive Papillary Carcinoma of the Breast Presenting as Post-Traumatic Recurrent Hemorrhagic Cysts
- A Case of Low-grade Papillary Adenocarcinoma of the Nasopharynx
- Primary Appendiceal Papillary Adenocarcinoma of Colonic Type: Report of a case
