Initial stage of fetal development of the pharyngotympanic tube cartilage with special reference to muscle attachments to the tube
- Affiliations
-
- 1Division of Otorhinolaryngology, Sendai Municipal Hospital, Sendai, Japan. entsendai@yahoo.co.jp
- 2Department of Anatomy and Embryology II, Faculty of Medicine, Complutense University, Madrid, Spain.
- 3Division of Internal Medicine, Iwamizawa Kojin-kai Hospital, Iwamizawa, Japan.
- 4Laboratory of Rehabilitative Auditory Science, Tohoku University Graduate School of Biomedical Engineering, Sendai, Japan.
- 5Department of Otolaryngology-Head and Neck Surgery, Tohoku University Graduate School of Medicine, Sendai, Japan.
- KMID: 2046746
- DOI: http://doi.org/10.5115/acb.2012.45.3.185
Abstract
- Fetal development of the cartilage of the pharyngotympanic tube (PTT) is characterized by its late start. We examined semiserial histological sections of 20 human fetuses at 14-18 weeks of gestation. As controls, we also observed sections of 5 large fetuses at around 30 weeks. At and around 14 weeks, the tubal cartilage first appeared in the posterior side of the pharyngeal opening of the PTT. The levator veli palatini muscle used a mucosal fold containing the initial cartilage for its downward path to the palate. Moreover, the cartilage is a limited hard attachment for the muscle. Therefore, the PTT and its cartilage seemed to play a critical role in early development of levator veli muscle. In contrast, the cartilage developed so that it extended laterally, along a fascia-like structure that connected with the tensor tympani muscle. This muscle appeared to exert mechanical stress on the initial cartilage. The internal carotid artery was exposed to a loose tissue facing the tubal cartilage. In large fetuses, this loose tissue was occupied by an inferior extension of the temporal bone to cover the artery. This later-developing anterior wall of the carotid canal provided the final bony origin of the levator veli palatini muscle. The tubal cartilage seemed to determine the anterior and inferior margins of the canal. Consequently, the tubal cartilage development seemed to be accelerated by a surrounding muscle, and conversely, the cartilage was likely to determine the other muscular and bony structures.
Keyword
MeSH Terms
Figure
-
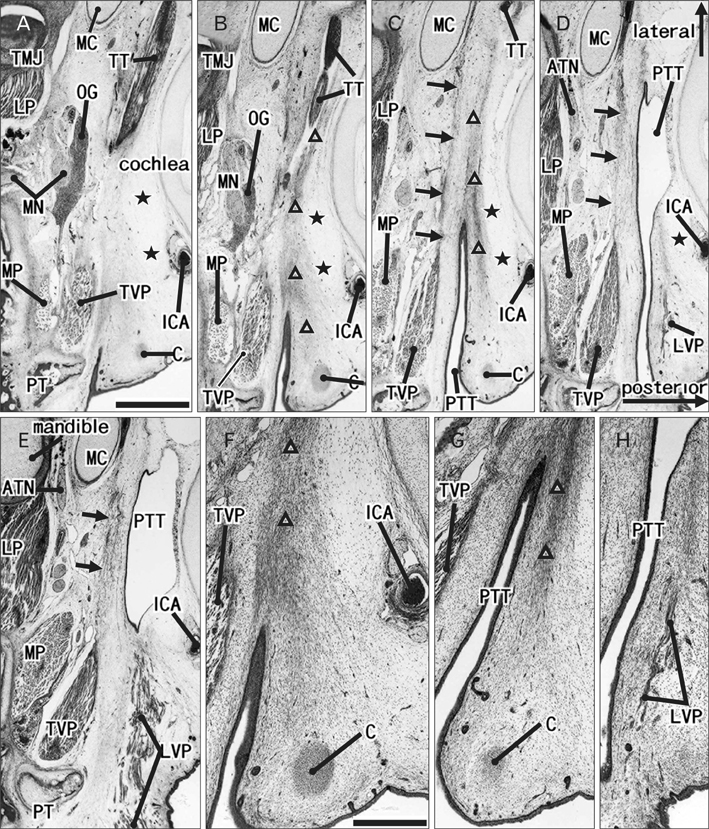
Fig. 1 Initial stage of development of the pharyngotympanic tube cartilage: a fetus with 102 mm crown-rump length. Hematoxlyin and eosin staining. Horizontal sections. (A [E]) is the most superior (or inferior) side of the figure: the distance is 3 mm. The posterior or lateral orientation is shown by arrows in (D). (F-H) are higher-magnigfication views of the pharyngotympanic tube (PTT) shown in (B-D), respectively. (A [C]) displays the superior (or inferior) end of the tubal cartilage (C): thus, the initial cartilage, almost 1 mm in diameter, is restricted to the posterior side of the pharyngeal opening of the PTT. The superior end of the levator veli palatini muscle (LVP) is seen 1 mm below the cartilage (D). A thick, band-like mesenchymal condensation or an "adventitia" in the text (triangles) extends between the cartilage and the tensor tympani muscle (TT). A facia (arrows) connects between the tensor veli palatini muscle (TVP) and Meckel's cartilage (MC). The internal cartotid artery (ICA) does not run through the bony carotid canal but is exposed to a large loose space (stars) on the posterior side of the PTT. ATN, auriculotemporal nerve; LP, lateral pterygoid muscle; MN, mandibular nerver; MP, medial pterygoid muscle; OG, otic ganglion; PT, pterygoid process; TMJ, temporomandibular joint. Scale bars in (A)=1 mm (A-E); in (F)=0.5 mm (F-H).
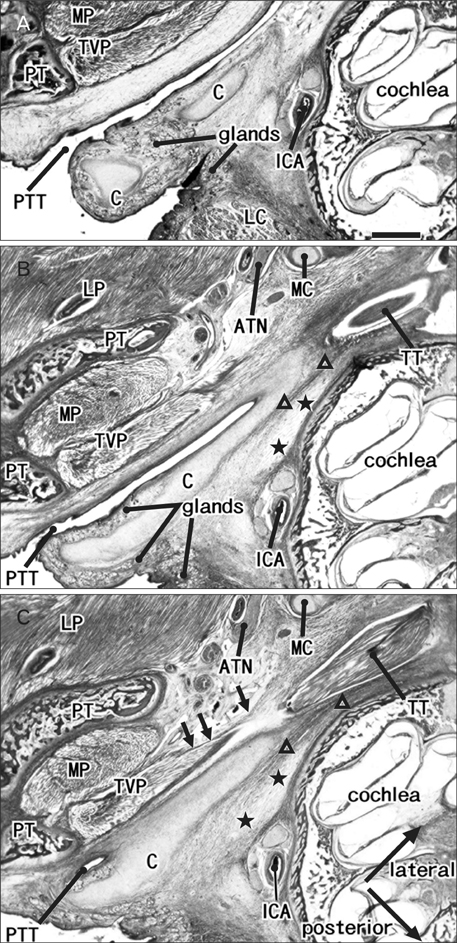
Fig. 2 (A-C) Laterally extending cartilage and the tensor tympani muscle in a crown-rump length 150-mm fetus. Hematoxylin and eosin staining. Horizontal sections. (A [C]) is the most inferior (or superior) side of the figure: the distance is 2 mm. The posterior or lateral orientation is shown by the arrows in (C). The cartilage (C) of the pharyngotympanic tube (PTT) extends along a fascial structure or an adventitia (triangles) that connects with the tensor tympani muscle (TT). Arrows indicate another fascia connecting between the tensor veli palatini muscle (TVP) and Meckel's cartilage (MC). The internal cartotid artery (ICA) is exposed to a loose space (stars) on the posterior side of the PTT. ATN, auriculotemporal nerve; LC, longus capitis muscle; LP, lateral pterygoid muscle; MP, medial pterygoid muscle; PT, pterygoid process. Scale bar=1 mm (A-C).
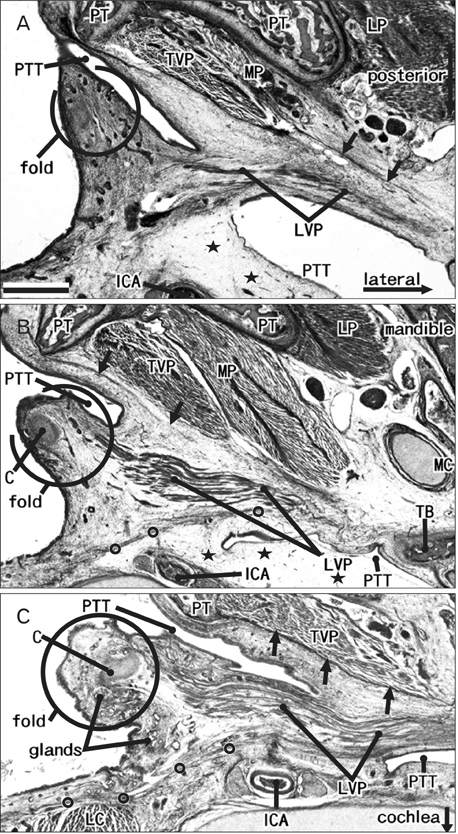
Fig. 3 Mucosal fold of the lateral pharyngeal wall and pharyngotympanic tube cartilage: three fetuses. Azan staining. Horizontal sections. All panels exhibit the inferior part or wall of the pharyngotympanic tube (PTT). The cartilage has not yet appeared in the specimen shown in (A) (crown-rump length [CRL], 101 mm), but the levator veli palatini muscle (LVP) has begun to extend into the putative mucosal fold at the pharyngeal opening of the PTT. In (B) (CRL, 100 mm) and (C) (CRL, 116 mm), the tubal cartilage (C) is almost 2 mm in length and these panels show the medial end. The LVP employs the mucosal fold containing the cartilage to guide its downward path to the palate. A fascia (circles), along the LVP, extends posteromedially to cover the longus capitis muscle (LC, panel C). Arrows indicate another fascia along the tensor veli palatini muscle (TVP). The internal cartotid artery (ICA) is exposed to a loose space (stars) on the posterior side of the PTT. LP, lateral pterygoid muscle; MP, medial pterygoid muscle; PT, pterygoid process;TB, temporal bone. Scale bar=1 mm (A-C).
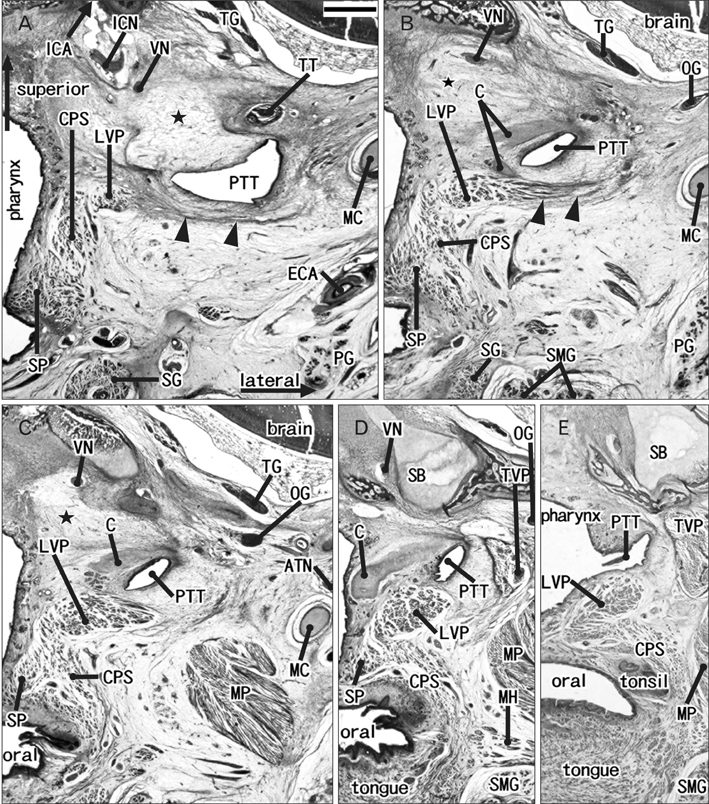
Fig. 4 Pharyngotympanic tube and the levator veli palatini muscle in a crown-rump length 125-mm fetus. Hematoxylin and eosin staining. Frontal sections. (A [E]) is the most posterior (or anterior) side of the figure: the distance is 3.3 mm. The superior or lateral orientation is shown by arrows in (A). The internal carotid artery (ICA with arrow) enters the brain cavity immediately posterior to (A). (A) and (B) display the most superior part or the origin (arrowheads) of the levator veli palatini muscle (LVP): because of the lack of a bony structure (star) near the pharyngotympanic tube (PTT), the origin has not yet become attached to the temporal bone, but extends along the inferior aspect of the PTT. The tubal cartilage (C) is divided into two fragments in (B). The levator muscle extends anteriorly along the inferior aspect of the PTT and its cartilage (C-E). ATN, auriculotemporal nerve; CPS, constrictor pharyngis superior muscle; ECA, external carotid artery; ICN, internal carotid nerve; MC, Meckel's cartilage; MH, mylohyoideus muscle; MP, medial pterygoid muscle; OG, otic ganglion; PG, parotid gland; SB, sphenoid bone (body); SG, styloglossus muscle; SMG, submandibular gland; SP, salpingopharyngeus muscle; TG, trigeminal nerve ganglion; TT, tensor tympani muscle; TVP, tensor veli palatini muscle; VN, Vidian's nerve (nerve of the pterygoid canal). Scale bar=1 mm (A-E).
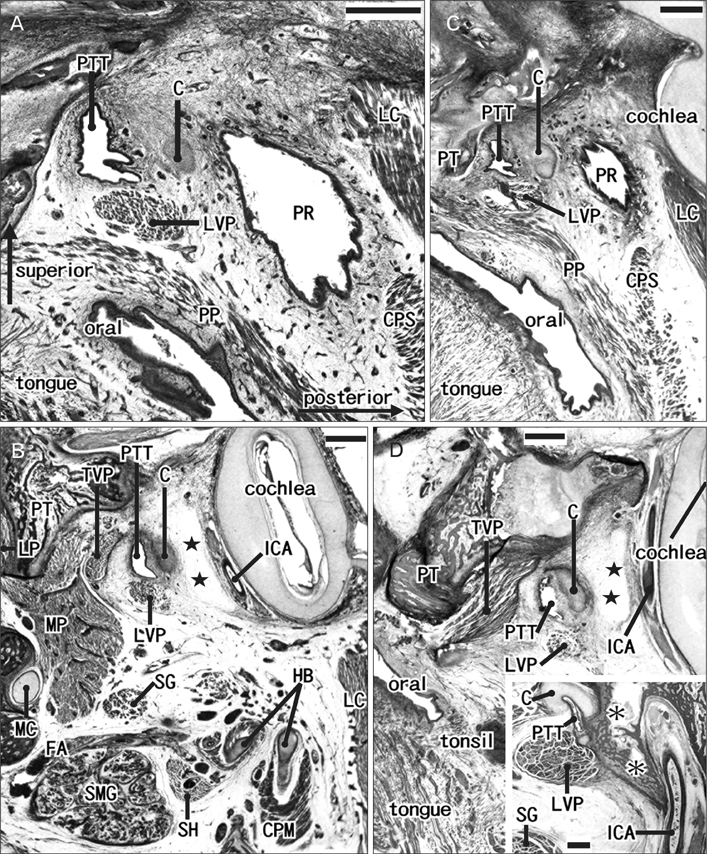
Fig. 5 Pharyngeal recess and the pharyngotympanic tube cartilage: two fetuses. Azan staining. Sagittal sections. (A and B [or C and D]) display fetuses with a crown-rump length of 103 mm (or 100 mm). (A) and (C) are located medially to (B) and (D), respectively. The superior or posterior orientation is shown by arrows in (A). The pharyngotympanic tube (PTT) and the tubal cartilage (C) are located between the pharyngeal recess (PR) and the PTT (A, B). Instead of the bony carotid canal, a loose space (stars in B and D) is evident between the PTT cartilage and the cochlea. Thus, the internal carotid artery (ICA) is exposed to the loose space. An inset (lower angle of D) displays a control specimen (30 wk) in which the bony carotid canal is established: the levator veli palatini muscle (LVP) attaches to the bony part that develops later (asterisks). CPM, constrictor pharyngis medius muscle; CPS, constrictor pharyngis superior muscle; FA, facial artery; HB, hyoid bone; LC, longus capitis muscle; LP, lateral pterygoid muscle; MC, Meckel's cartilage; MP, medial pterygoid muscle; PP, palatopharyngeal muscle; PT, pterygoid process; SG, styloglossus muscle; SH, stylohyoid muscle; SMG, submandibular gland; TVP, tensor veli palatini muscle. Scale bars=1 mm (A-D, inset in D).
Cited by 1 articles
-
Fetal development of the carotid canal with special reference to a contribution of the sphenoid bone and pharyngotympanic tube
Yohei Honkura, Masahito Yamamoto, José Francisco Rodríguez-Vázquez, Gen Murakam, Hiroshi Abe, Shin-ichi Abe, Yukio Katori
Anat Cell Biol. 2021;54(2):259-269. doi: 10.5115/acb.20.310.
Reference
-
1. Katori Y, Rodríguez-Vázquez JF, Kawase T, Murakami G, Cho BH, Abe S. Early fetal development of hard tissue pulleys for the human superior oblique and tensor veli palatini muscles. Ann Anat. 2011. 193:127–133.2. Katori Y, Takeuchi H, Rodríguez-Vázquez JF, Kitano H, Murakami G, Kawase T. Fetal development of the human epiglottis revisited: appearance of GFAP-positive mesenchymal cells and fibrous connections with other laryngeal and lingual structures. Ann Anat. 2011. 193:149–155.3. Swarts JD, Rood SR, Doyle WJ. Fetal development of the auditory tube and paratubal musculature. Cleft Palate J. 1986. 23:289–311.4. Couly G, Grapin-Botton A, Coltey P, Ruhin B, Le Douarin NM. Determination of the identity of the derivatives of the cephalic neural crest: incompatibility between Hox gene expression and lower jaw development. Development. 1998. 125:3445–3459.5. Ruhin B, Creuzet S, Vincent C, Benouaiche L, Le Douarin NM, Couly G. Patterning of the hyoid cartilage depends upon signals arising from the ventral foregut endoderm. Dev Dyn. 2003. 228:239–246.6. Santagati F, Minoux M, Ren SY, Rijli FM. Temporal requirement of Hoxa2 in cranial neural crest skeletal morphogenesis. Development. 2005. 132:4927–4936.7. Minoux M, Antonarakis GS, Kmita M, Duboule D, Rijli FM. Rostral and caudal pharyngeal arches share a common neural crest ground pattern. Development. 2009. 136:637–645.8. Rodríguez-Vázquez JF, Murakami G, Verdugo-López S, Abe S, Fujimiya M. Closure of the middle ear with special reference to the development of the tegmen tympani of the temporal bone. J Anat. 2011. 218:690–698.9. Plank J, Rychlo A. A method for quick decalcification. Zentralbl Allg Pathol. 1952. 89:252–254.10. Khoo FY, Kanagasuntheram R, Chia KB. Variations of the lateral recesses of the nasopharynx. Arch Otolaryngol. 1967. 86:456–462.11. Hayes MA. Abdominopelvic fasciae. Am J Anat. 1950. 87:119–161.12. Matsubara A, Murakami G, Niikura H, Kinugasa Y, Fujimiya M, Usui T. Development of the human retroperitoneal fasciae. Cells Tissues Organs. 2009. 190:286–296.13. Miyake N, Hayashi S, Kawase T, Cho BH, Murakami G, Fujimiya M, Kitano H. Fetal anatomy of the human carotid sheath and structures in and around it. Anat Rec (Hoboken). 2010. 293:438–445.14. Abe M, Murakami G, Noguchi M, Kitamura S, Shimada K, Kohama GI. Variations in the tensor veli palatini muscle with special reference to its origin and insertion. Cleft Palate Craniofac J. 2004. 41:474–484.15. Rohan RF, Turner L. The levator palati muscle. J Anat. 1956. 90:153–154.16. Klueber K, Langdon HL. Anatomy of musculus levator veli palatini in the 15-week human fetus. Acta Anat (Basel). 1979. 105:94–105.17. Doyle WJ, Kitajiri M, Sando I. The anatomy of the auditory tube and paratubal musculature in a one month old cleft palate infant. Cleft Palate J. 1983. 20:218–226.18. Takasaki K, Sando I, Balaban CD, Ishijima K. Postnatal development of eustachian tube cartilage. A study of normal and cleft palate cases. Int J Pediatr Otorhinolaryngol. 2000. 52:31–36.19. Mallo M, Schrewe H, Martin JF, Olson EN, Ohnemus S. Assembling a functional tympanic membrane: signals from the external acoustic meatus coordinate development of the malleal manubrium. Development. 2000. 127:4127–4136.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Immunohistochemical Localization of Insulin-Like Growth Factor-I in the Eustachian Tube of the Rat
- Unilateral Vocal Cord Palsy after Endotracheal Intubation: A case report
- Fetal development of the carotid canal with special reference to a contribution of the sphenoid bone and pharyngotympanic tube
- Comment on: Trans-Tympanic Cartilage Chip Insertion for Intractable Patulous Eustachian Tube
- The Morphologic Study of Elastic Structures in the Developing Murine Eustachian Tube
