J Korean Fract Soc.
2015 Apr;28(2):103-109. 10.12671/jkfs.2015.28.2.103.
Treatment of the Femoral Fracture Using Sirus(R) Nail: A Comparison of Complication according to the Entry Potal
- Affiliations
-
- 1Department of Orthopaedic Surgery, Kwangju Christian Hospital, Gwangju, Korea. paedic@chol.com
- KMID: 2044017
- DOI: http://doi.org/10.12671/jkfs.2015.28.2.103
Abstract
- PURPOSE
The purpose of this study is to analyze the clinical results of fixation using Sirus(R) nail in patients with femoral subtrochanteric and shaft fracture and the difference in the frequency of complications according to the entry portal.
MATERIALS AND METHODS
From July 2006 to August 2013, at least 1-year clinical follow-up, we retrospectively analyzed 36 cases with femoral subtrochanteric (15 cases) and shaft fracture (21 cases) who underwent surgery using Sirus(R) nail. We reviewed the records of operation time, intra-operative amounts of bleeding and complications. At last follow-up, we reviewed clinical results by Ray-Sanders criteria and analyzed the periods of bone union on the radiograph. We also measured changing of the femoral neck-shaft angle in the subtrochanteric fractures and angulation in the shaft fractures, respectively. Considering anatomical variation of the trochanter and fracture position of subtrochanteric and femoral shaft, entry points were divided into subgroups, and the clinical results were compared.
RESULTS
The mean Ray-Sanders score was 27.4, 27 cases (75.0%) were good or excellent. The mean periods of bone union was 21.1 weeks in 31 cases. The mean neck-shaft angles were 135.7o preoperatively, 130.2o postoperatively. The mean angulation of the femur was 24.4o preoperatively, 2.4o postoperatively in patients of femoral shaft fractures. Despite no statistical significance, greater trochanter tip entry point and lateral entry point had a higher rate of frequency than medial entry point, with respect to the occurrence of iatrogenic fracture and malalignment.
CONCLUSION
Using Sirus(R) nail for femoral subtrochanteric and shaft fractures showed good clinical and radiographic results and a high rate of union. Medial entry point yielded slightly better results in the occurrence of iatrogenic fracture and malalignment, compared to greater trochanter tip entry point and lateral entry point.
Keyword
MeSH Terms
Figure
-
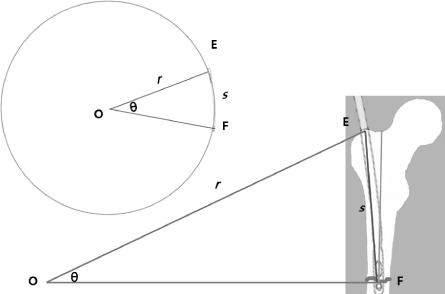
Fig. 1 For estimation of proper entry portals, we assumed the length of Sirus® nail (s) to circular arc (EF). The radius (r) of the circle was informed by regular manufacturer's information. Finally we estimated the central angle (θ) from the circle and compared with contralateral neck-shaft angle.

Fig. 2 Illustration of subdivision by entry points. ①: Lateral entry point, ②: greater trochanter tip entry point, ③: medial entry point.

Fig. 3 Preoperative and postoperative antero-posterior view of iatrogenic fracture that occurred in Sirus® nail insertion using lateral entry point.
Reference
-
1. Winquist RA, Hansen ST Jr, Clawson DK. Closed intramedullary nailing of femoral fractures. A report of five hundred and twenty cases. J Bone Joint Surg Am. 1984; 66:529–539.
Article2. Mileski RA, Garvin KL, Crosby LA. Avascular necrosis of the femoral head in an adolescent following intramedullary nailing of the femur. A case report. J Bone Joint Surg Am. 1994; 76:1706–1708.
Article3. Khan FA, Ikram MA, Badr AA, al-Khawashki H. Femoral neck fracture: a complication of femoral nailing. Injury. 1995; 26:319–321.
Article4. Dora C, Leunig M, Beck M, Rothenfluh D, Ganz R. Entry point soft tissue damage in antegrade femoral nailing: a cadaver study. J Orthop Trauma. 2001; 15:488–493.
Article5. Ansari Moein CM, Verhofstad MH, Bleys RL, van der Werken C. Soft tissue injury related to choice of entry point in antegrade femoral nailing: piriform fossa or greater trochanter tip. Injury. 2005; 36:1337–1342.
Article6. Yun HH, Oh CH, Yi JW. Subtrochanteric femoral fracture during trochanteric nailing for the treatment of femoral shaft fracture. Clin Orthop Surg. 2013; 5:230–234.
Article7. Afsari A, Liporace F, Lindvall E, Infante A Jr, Sagi HC, Haidukewych GJ. Clamp-assisted reduction of high subtrochanteric fractures of the femur. J Bone Joint Surg Am. 2009; 91:1913–1918.
Article8. Lakhwani OP. Correlation of trochanter-shaft angle in selection of entry site in antegrade intramedullary femoral nail. ISRN Orthop. 2012; 2012:1–5.
Article9. Wiss DA, Brien WW, Stetson WB. Interlocked nailing for treatment of segmental fractures of the femur. J Bone Joint Surg Am. 1990; 72:724–728.
Article10. Sanders R, Swiontkowski M, Rosen H, Helfet D. Double-plating of comminuted, unstable fractures of the distal part of the femur. J Bone Joint Surg Am. 1991; 73:341–346.
Article11. Ha SH, Kim WH, Lee GC. Results of intramedullary nailing of femoral shaft fracture: trochanteric entry portal (Sirus nail) versus piriformis entry portal (M/DN nail). J Korean Fract Soc. 2014; 27:50–57.
Article12. Ostrum RF, Marcantonio A, Marburger R. A critical analysis of the eccentric starting point for trochanteric intramedullary femoral nailing. J Orthop Trauma. 2005; 19:681–686.
Article13. Ricci WM, Bellabarba C, Lewis R, et al. Angular malalignment after intramedullary nailing of femoral shaft fractures. J Orthop Trauma. 2001; 15:90–95.
Article14. Linke B, Ansari Moein C, Bösl O, et al. Lateral insertion points in antegrade femoral nailing and their influence on femoral bone strains. J Orthop Trauma. 2008; 22:716–722.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Results of Intramedullary Nailing of Femoral Shaft Fracture: Trochanteric Entry Portal (Sirus Nail) versus Piriformis Entry Portal (M/DN Nail)
- Failure to Remove a Trochanteric Entry Femoral Nail and Its Cause in Adolescent Patients: Two Cases Report
- Comparison of Greater Trochanter Versus Piriformis Entry Nail for Treatment of Femur Shaft Fracture
- Bursting Fracture of the Proximal Femur during Insertion of Unreamed Femoral Nail for Femur Shaft Fracture: A Case Report
- Retrieval of a Broken Intramedullary Nail after Refracture of Femoral Shaft: A case report
