Results of Intramedullary Nailing of Femoral Shaft Fracture: Trochanteric Entry Portal (Sirus Nail) versus Piriformis Entry Portal (M/DN Nail)
- Affiliations
-
- 1Department of Orthopaedic Surgery, School of Medicine, Chosun University, Gwangju, Korea. leekci@chosun.ac.kr
- KMID: 1817002
- DOI: http://doi.org/10.12671/jkfs.2014.27.1.50
Abstract
- PURPOSE
To compare treatment results obtained using the trochanteric (Sirus nail) entry portal with those obtained using the Piriformis fossa (M/DN) entry portal during intramedullary (IM) nailing of femur shaft fractures.
MATERIALS AND METHODS
Four hundreds and thirty-two patients treated for femur shaft fracture using IM nails from February, 2001 to May, 2010 were divided into two groups. group 1 was composed of 180 patients treated through the trochanteric (Sirus nail; n=180) entry portal, while group 2 contained 170 patients treated through the piriformis fossa (M/DN nail; n=170) entry portal. We compared the clinical and radiographic findings of both groups to evaluate the treatment results.
RESULTS
Functional result, range of motion and union time (18, 20 weeks) were similar in both groups. The operation time of patients in the over-weighted group was 90 minutes in group 1 and 120 minutes in group 2 (p<0.05). Additionally, the blood loss was 280 ml in group 1 and 335 ml in group 2, and in case of over-weight patients, group 2 showed more blood loss (p<0.05). The duration of exposure to fluoroscopy differed slightly, with group 1 being less exposed than group 2; however, this difference was not significant (p>0.05). There were 18 iatrogenic fractures in group 1 and 4 in group 2 (p<0.05).
CONCLUSION
There was not much difference in complications based on clinical and radiographic findings of both groups. For groups using the trochanteric entry portal, the operation time was shorter and blood loss was lower than in groups using the piriformis entry portal. Iatrogenic fracture occurred more often in the group using the trochanteric entry portal than in the group using the piriformis entry portal.
Keyword
MeSH Terms
Figure
-
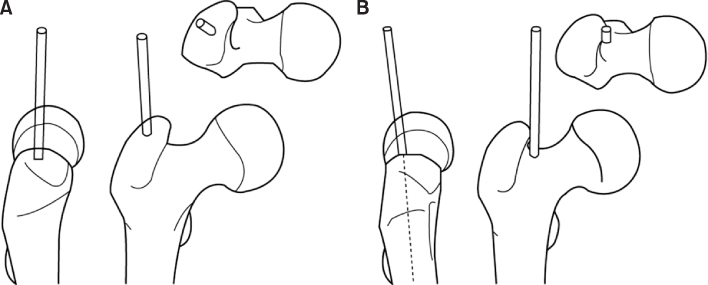
Fig. 1 (A) Trochanteric entry portal: the correct location for the trochanteric entry point immediately next to the tip of the greater trochanter on the anteroposterior view and exactly centered on the axial view. (B) Piriformis entry point: the correct position for the piriformis fossa entry point is immediately medial to the tip of the greater trochanter.
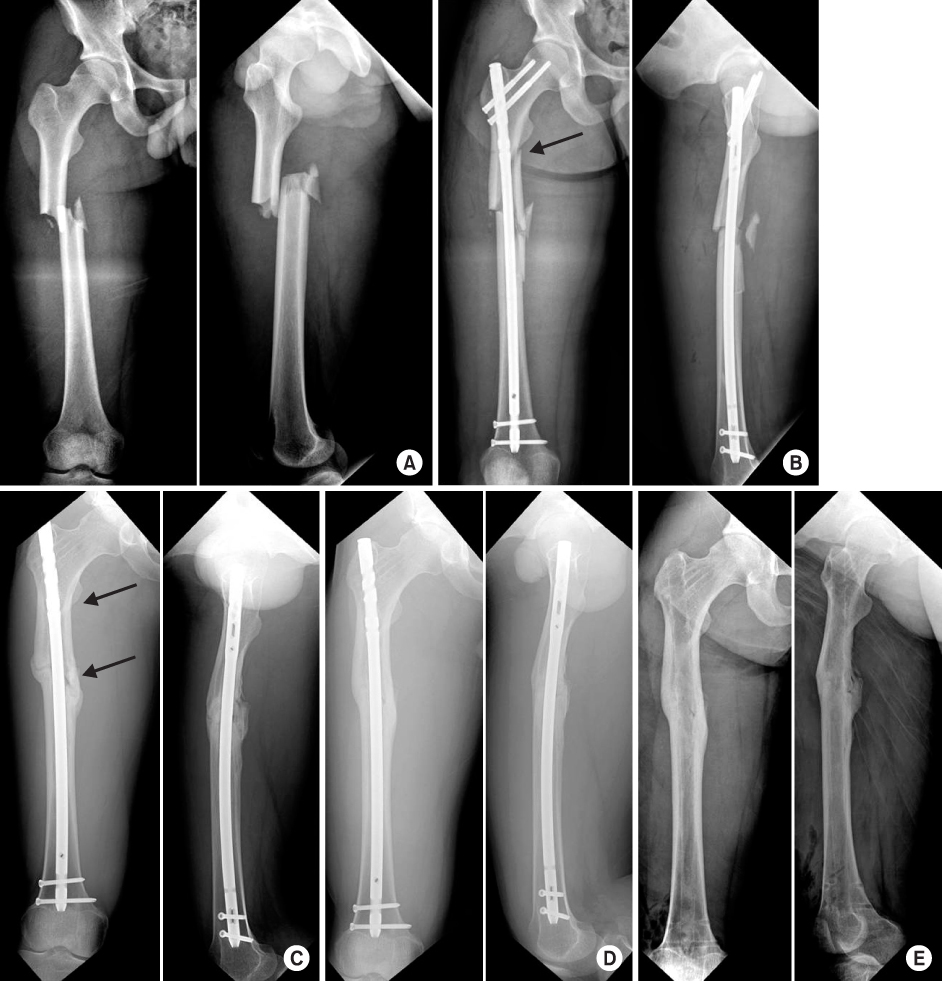
Fig. 2 (A) Anteroposterior and lateral radiograph of a 21-year-old male who received a femur midshaft fracture in a traffic accident. (B) Postoperative radiograph: iatrogenic fracture (arrow) during closed nailing of the femoral shaft fracture via the trochanteric tip. (C) Anteroposterior and lateral radiographs of femoral diaphyseal nonunion after 4 months. Nail dynamization was performed, femoral diaphyseal nonunion (arrows). (D) Bone union observed on radiographs taken 2 years after operation. (E) After implant removal.
Cited by 3 articles
-
Comparison of Greater Trochanter Versus Piriformis Entry Nail for Treatment of Femur Shaft Fracture
Jong-Hee Lee, Jong-Hoon Park, Si-Yeong Park, Seong-Cheol Park, Seung-Beom Han
J Korean Fract Soc. 2014;27(4):287-293. doi: 10.12671/jkfs.2014.27.4.287.Treatment of the Femoral Fracture Using Sirus® Nail: A Comparison of Complication according to the Entry Potal
Young-Yool Chung, Dong-Hyuk Choi, Dae-Hyun Yoon, Jung-Ho Lee, Ji-Hun Park
J Korean Fract Soc. 2015;28(2):103-109. doi: 10.12671/jkfs.2015.28.2.103.Failure to Remove a Trochanteric Entry Femoral Nail and Its Cause in Adolescent Patients: Two Cases Report
Ji-Hwan Kim, Seung-Oh Nam, Young-Soo Byun, Han-Sang Kim
J Korean Fract Soc. 2015;28(1):71-76. doi: 10.12671/jkfs.2015.28.1.71.
Reference
-
1. Ansari Moein CM, Verhofstad MH, Bleys RL, van der Werken C. Soft tissue injury related to choice of entry point in antegrade femoral nailing: piriform fossa or greater trochanter tip. Injury. 2005; 36:1337–1342.
Article2. Bohler L, Bohler J. Kütscher's medullary nailing. J Bone Joint Surg Am. 1949; 31A:295–305.3. Gausepohl T, Pennig D, Koebke J, Harnoss S. Antegrade femoral nailing: an anatomical determination of the correct entry point. Injury. 2002; 33:701–705.
Article4. Harper MC, Carson WL. Curvature of the femur and the proximal entry point for an intramedullary rod. Clin Orthop Relat Res. 1987; (220):155–161.
Article5. Johnson KD, Tencer AF, Sherman MC. Biomechanical factors affecting fracture stability and femoral bursting in closed intramedullary nailing of femoral shaft fractures, with illustrative case presentations. J Orthop Trauma. 1987; 1:1–11.
Article6. Kempf I, Grosse A, Beck G. Closed locked intramedullary nailing. Its application to comminuted fractures of the femur. J Bone Joint Surg Am. 1985; 67:709–720.
Article7. Kim JW, Byun SE, Oh WH, Kim JJ. Bursting fracture of the proximal femur during insertion of unreamed femoral nail for femur shaft fracture: a case report. J Korean Fract Soc. 2010; 23:227–231.
Article8. Klemm K, Schellmann WD. Dynamic and static locking of the intramedullary nail. Monatsschr Unfallheilkd Versicher Versorg Verkehrsmed. 1972; 75:568–575.9. Küntscher G. Die Marknalung von Knochenbrüchen. Langenbecks Arch Klin Chir. 1940; 200:443–455.10. Küntscher G. A new method of treatment of pertrochanteric fractures. Proc R Soc Med. 1970; 63:1120–1121.11. Linke B, Ansari Moein C, Bösl O, et al. Lateral insertion points in antegrade femoral nailing and their influence on femoral bone strains. J Orthop Trauma. 2008; 22:716–722.
Article12. McKee MD, Waddell JP. Intramedullary nailing of femoral fractures in morbidly obese patients. J Trauma. 1994; 36:208–210.
Article13. Ostrum RF. A greater trochanteric insertion site for femoral intramedullary nailing in lipomatous patients. Orthopedics. 1996; 19:337–340.
Article14. Ostrum RF, Marcantonio A, Marburger R. A critical analysis of the eccentric starting point for trochanteric intramedullary femoral nailing. J Orthop Trauma. 2005; 19:681–686.
Article15. Ricci WM, Devinney S, Haidukewych G, Herscovici D, Sanders R. Trochanteric nail insertion for the treatment of femoral shaft fractures. J Orthop Trauma. 2005; 19:511–517.
Article16. Ricci WM, Schwappach J, Tucker M, et al. Trochanteric versus piriformis entry portal for the treatment of femoral shaft fractures. J Orthop Trauma. 2006; 20:663–667.
Article17. Robinson CM, Houshian S, Khan LA. Trochanteric-entry long cephalomedullary nailing of subtrochanteric fractures caused by low-energy trauma. J Bone Joint Surg Am. 2005; 87:2217–2226.
Article18. Stannard JP, Bankston L, Futch LA, McGwin G, Volgas DA. Functional outcome following intramedullary nailing of the femur: a prospective randomized comparison of piriformis fossa and greater trochanteric entry portals. J Bone Joint Surg Am. 2011; 93:1385–1391.19. Starr AJ, Hay MT, Reinert CM, Borer DS, Christensen KC. Cephalomedullary nails in the treatment of high-energy proximal femur fractures in young patients: a prospective, randomized comparison of trochanteric versus piriformis fossa entry portal. J Orthop Trauma. 2006; 20:240–246.
Article20. Tucker MC, Schwappach JR, Leighton RK, Coupe K, Ricci WM. Results of femoral intramedullary nailing in patients who are obese versus those who are not obese: a prospective multicenter comparison study. J Orthop Trauma. 2007; 21:523–529.
Article21. Winquist RA, Hansen ST Jr, Clawson DK. Closed intramedullary nailing of femoral fractures. A report of five hundred and twenty cases. J Bone Joint Surg Am. 1984; 66:529–539.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Treatment of IM Nailing of Femoral Shaft Fracture: Piriformis Fossa versus Trochanteric Entry Portal
- Comparison of Greater Trochanter Versus Piriformis Entry Nail for Treatment of Femur Shaft Fracture
- Treatment of the Femoral Fracture Using Sirus(R) Nail: A Comparison of Complication according to the Entry Potal
- Failure to Remove a Trochanteric Entry Femoral Nail and Its Cause in Adolescent Patients: Two Cases Report
- Percutaneous Interlocking Intramedullary Nailing of Femoral Shaft Fracture with Retrograde Guide Wire Insertion Technique
