Epidural Arteriovenous Fistula in the Cervical Spine Associated with Unilateral Upper Extremity Pain: A Case Report
- Affiliations
-
- 1Spine Center, Department of Orthopaedic Surgery, Sun General Hospital, Daejeon, Korea. hc5771@chollian.net
- KMID: 2040782
- DOI: http://doi.org/10.4184/jkss.2006.13.1.59
Abstract
- We experienced a rare case of an epidural arteriovenous fistula, which presented with symptoms similar to those of cervical radiculopathy. An 18-years-old woman suffered from neck pain, which radiated to the left upper extremity for 4 months. On neurologic examination, there were sensory impairments of the left C4 to C8 dermatomes and intermittent weakness in both lower extremities after exercise. An MRI of the cervical spine demonstrated a mass, which produced a serpentine-like signal void within the spinal canal from C1 to C7. The feeding artery of the fistula and the arterialized epidural venous plexus within the spinal canal were found on vertebral angiography. One year after an endovascular embolization with platinum coils, the clinical symptoms resolved and complete resolution of the arteriovenous fistula was confirmed by angiogram and MRI scan.
MeSH Terms
Figure
-
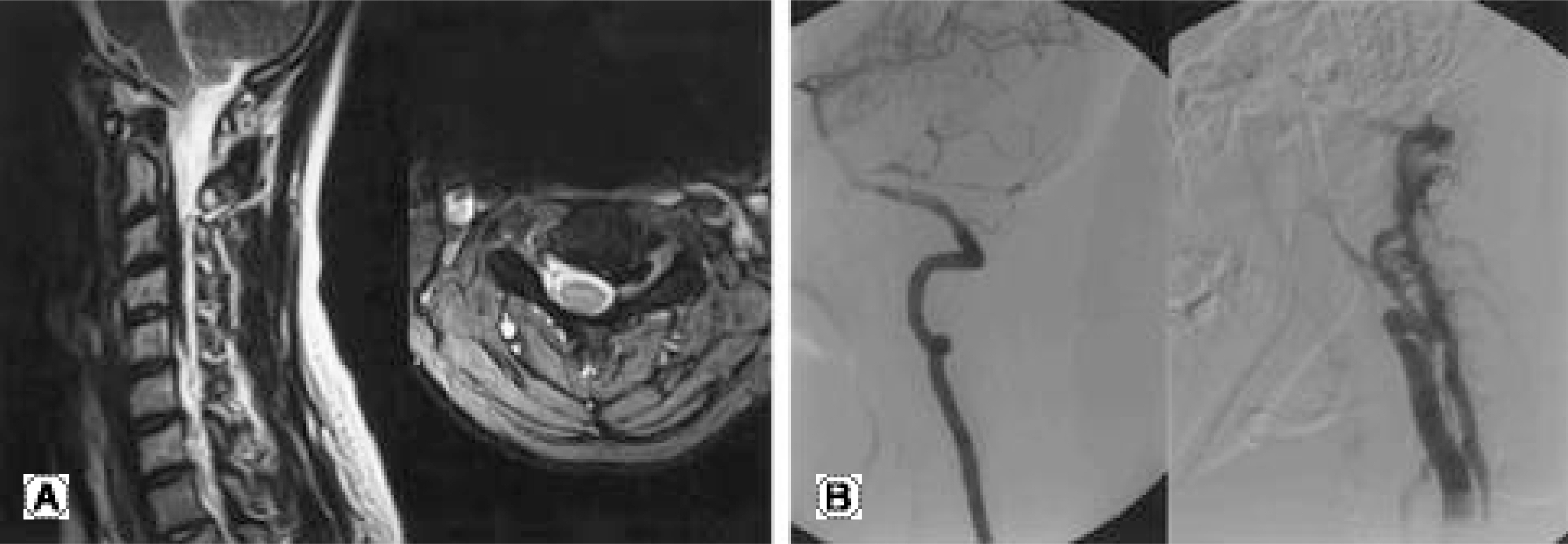
Fig. 1. (A) Pre-embolization MRI at C3-4 level. The cervical dura is compressed by dilated, engorged epidural veins and feeding artery is located in the left C 3-4 intervertebral foramen. (B) Left vertebral angiography shows cervical vascular abnormality comparing to normal right side vertebral artery.
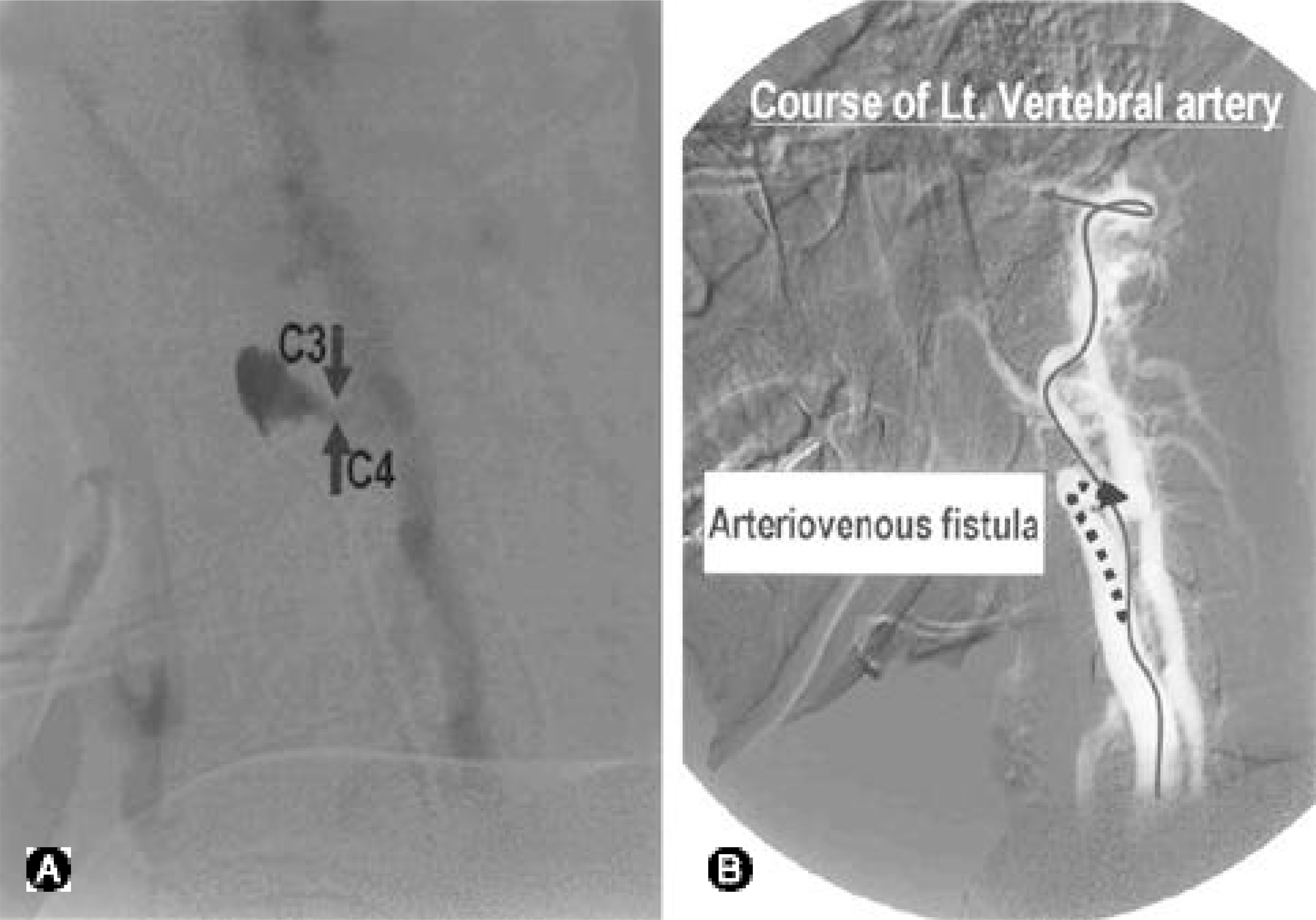
Fig. 2. (A) Abnormal fistular flow through feeding artery is shown at C3-4 intervertebral foramen. (B) Schematic drawings of the left vertebral angiogram.
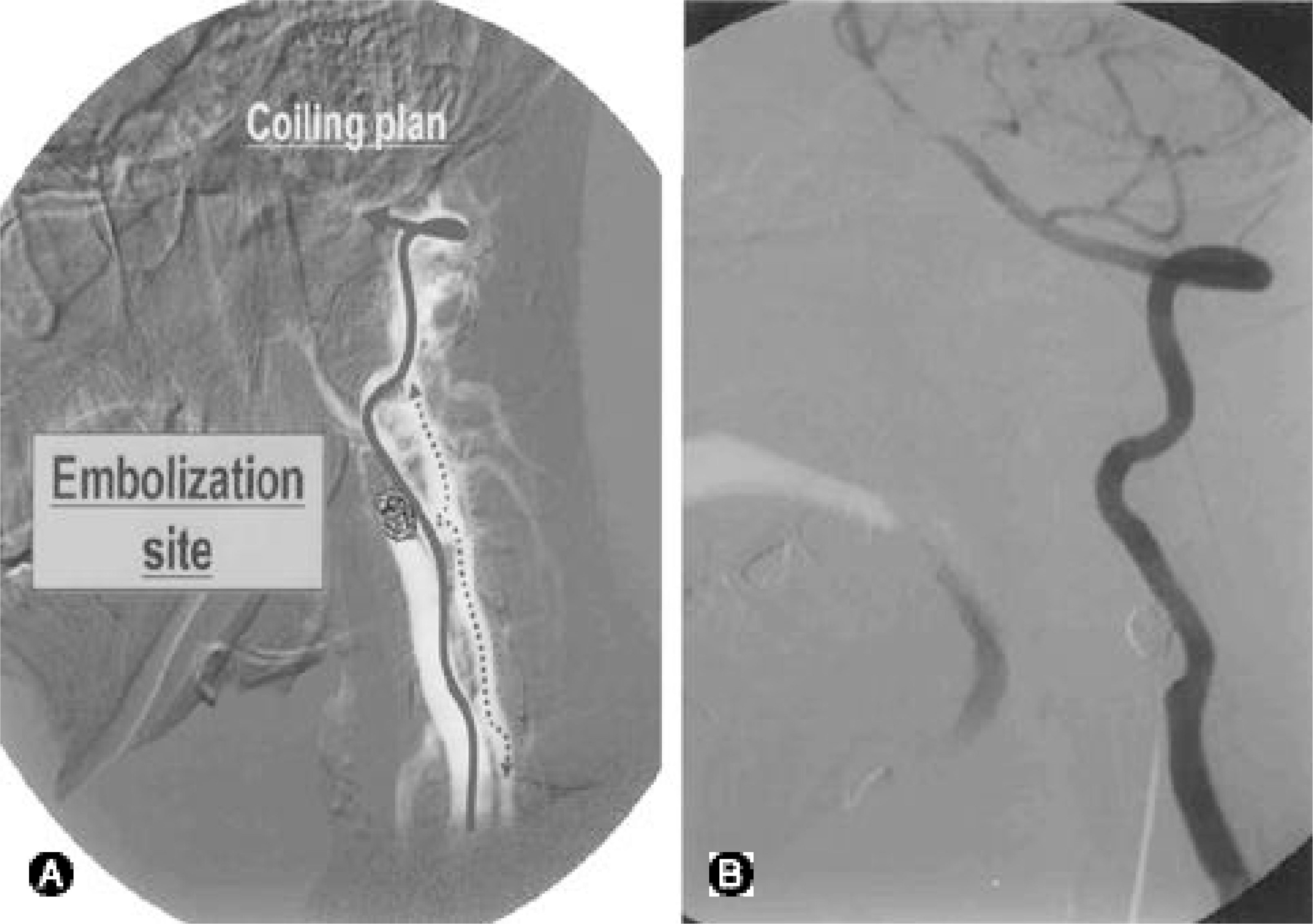
Fig. 3. (A) Schematic plan of the endovascular embolization with platinium coils. (B) Post-embolization angiography shows the complete loss of the extradural arteriovenous fistula and the preservation of left side vertebral artery.
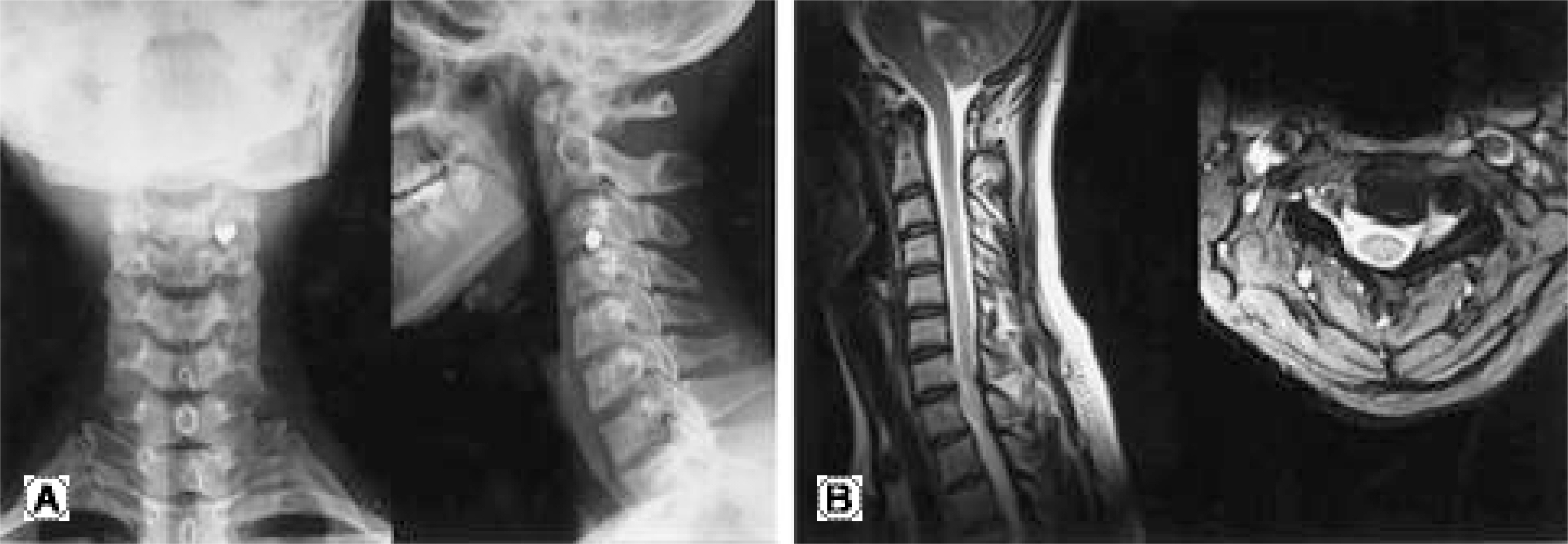
Fig. 4. (A) Postoperative cervical radiogram. (B) Postoperative cervical spine MRIs show the complete loss of the extradural arteriovenous fistula.
Reference
-
1). Spetzler RF. Spinal arteriovenous malformations. (cited from H.Richard Winn ed. Youmans Neurological Surgery. 5nd ed. Saunders:. 2381–22419. 2004.2). Spetzler RF, Detwiler PW. Modified classification of spinal cord vascular lesions. J Neurosurg (Spine 2). 2002; 96:145–156.
Article3). Oldfield E, Doppman J. Spinal arteriovenous malformations. Neurosurg. 1988; 34:161–183.4). Rosenblum B, Oldfield E, Doppman J. Spinal arteriovenous malformations: A comparison of dural arteriovenous fistulas and intradural AVMs in 81 patients. J Neurosurg. 1987; 67:795–802.
Article5). Afshar JKB, Doppman JL, Oldfield EH. Surgical inter -ruption of intradural draining vein as curative treatment of spinal dural arteriovenous fistulas. J Neurosurg. 1995; 82:196–200.6). Assai JC, Hayashi TC. Exclusively epidural arteriovenous fistula in the cervical spine with spinal cord symptoms. Case Report. Neurosurgery. 2001; 48:1372–1376.
Article7). Hassler W, Thron A. Flow velocity and pressure mea -surements in spinal dural arteriovenous fistulas. Neurosurg Rev. 1994; 17:29–36.8). Hassler W, Thron A, Grote EH. Hemodynamics of spinal dural arteriovenous fistulas: An interoperative study. J Neurosurg. 1989; 70:360–370.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endovascular Treatment of Spinal Dural and Epidural Arteriovenous Fistula as Complication of Lumbar Surgery
- Cervical Radiculopathy Caused by Spinal Epidural Arteriovenous Fistula (SEDAVF) Without Intradural Drainage: A Case Report and Literature Review
- Paraplegia following cervical epidural catheterization using loss of resistance technique with air: a case report
- Spinal Epidural Arteriovenous Fistula Presented with Subdural Hematoma: a Case of Transarterial Embolization Using NBCA
- Endovascular Treatment for Spontaneous Vertebral Arteriovenous Fistula in Neurofibromatosis Type 1: A Case Report
