Role of MRI and Plain Radiograph to Diagnose Fibrous Dysplasia Mimicking Metastasis on PET/CT in a Patient with Breast Cancer
- Affiliations
-
- 1Department of Radiology, St. Paul's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea.
- 2Department of Radiology, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea. whjee@catholic.ac.kr
- 3Department of Nuclear Medicine, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea.
- 4Department of Pathology, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea.
- 5Department of Orthopedic Surgery, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea.
- KMID: 2006342
- DOI: http://doi.org/10.5292/jkbjts.2010.16.1.47
Abstract
- Fibrous dysplasia is a common benign disorder of bone in which normal bone marrow is replaced with fibro-osseous tissue. As PET/CT is increasingly used for the staging of different malignant disease, incidentally found fibrous dysplasia with increased FDG uptake may mimic metastasis. We report on a 46-year-old woman with fibrous dysplasia who underwent PET/CT because of suspected recurrence of breast cancer and was misdiagnosed as a bony metastasis with a focal FDG uptake on left proximal femur. This lesion was interpreted as fibrous dysplasia based on MRI in addition to the plain radiographs. We conclude that MRI in addition to radiography may help to differentiate fibrous dysplasia mimicking metastasis on PET/CT in the patients with malignancy.
Keyword
MeSH Terms
Figure
-
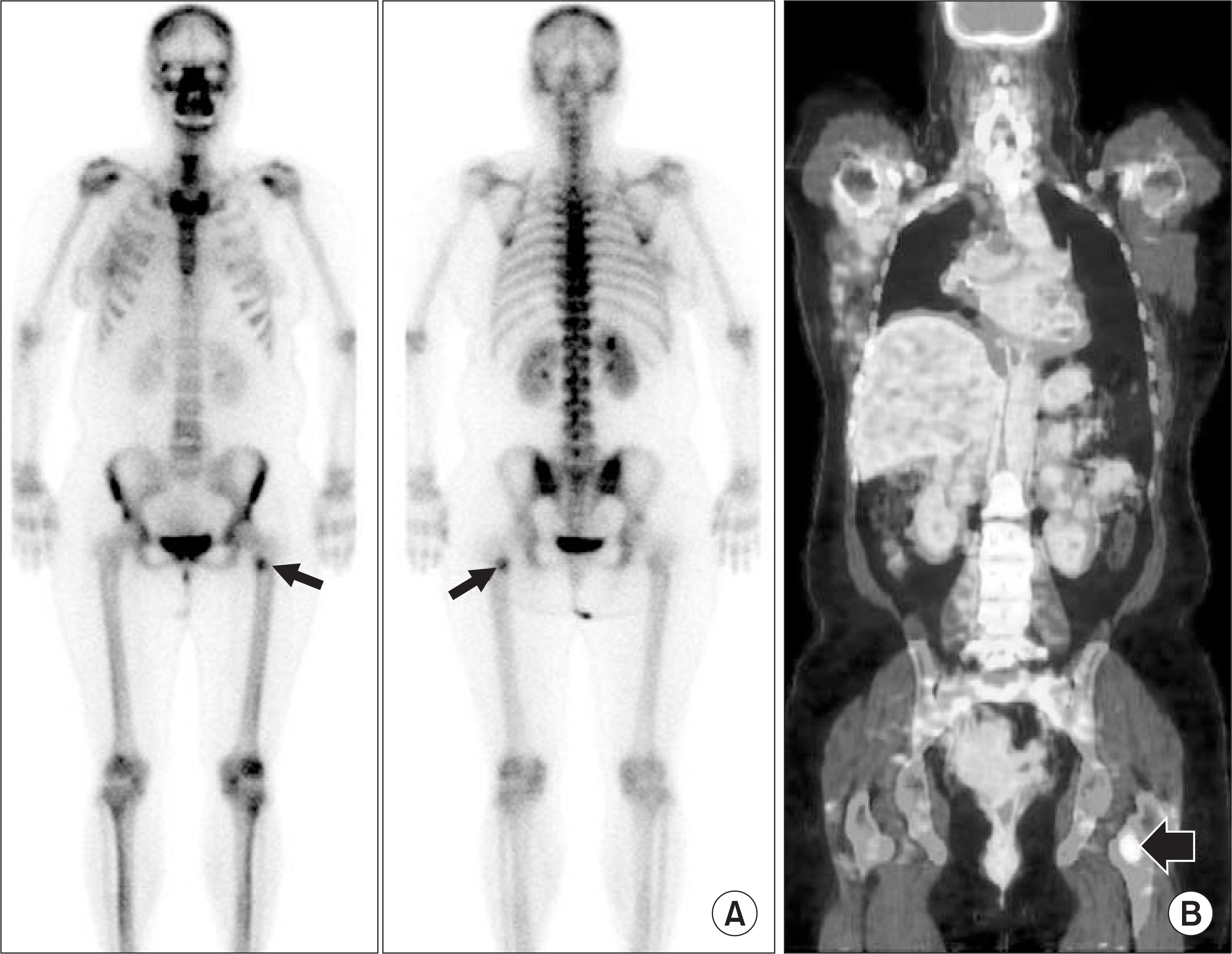
Figure 1. A 46-year-old woman with breast cancer. Bone scintigraphy (A) shows a focal hot uptake (arrow) in left proximal femur. PET/CT (B) shows a focal FDG uptake (arrow) in left proximal femur and was mis-interpreted as a single metastasis from breast cancer.
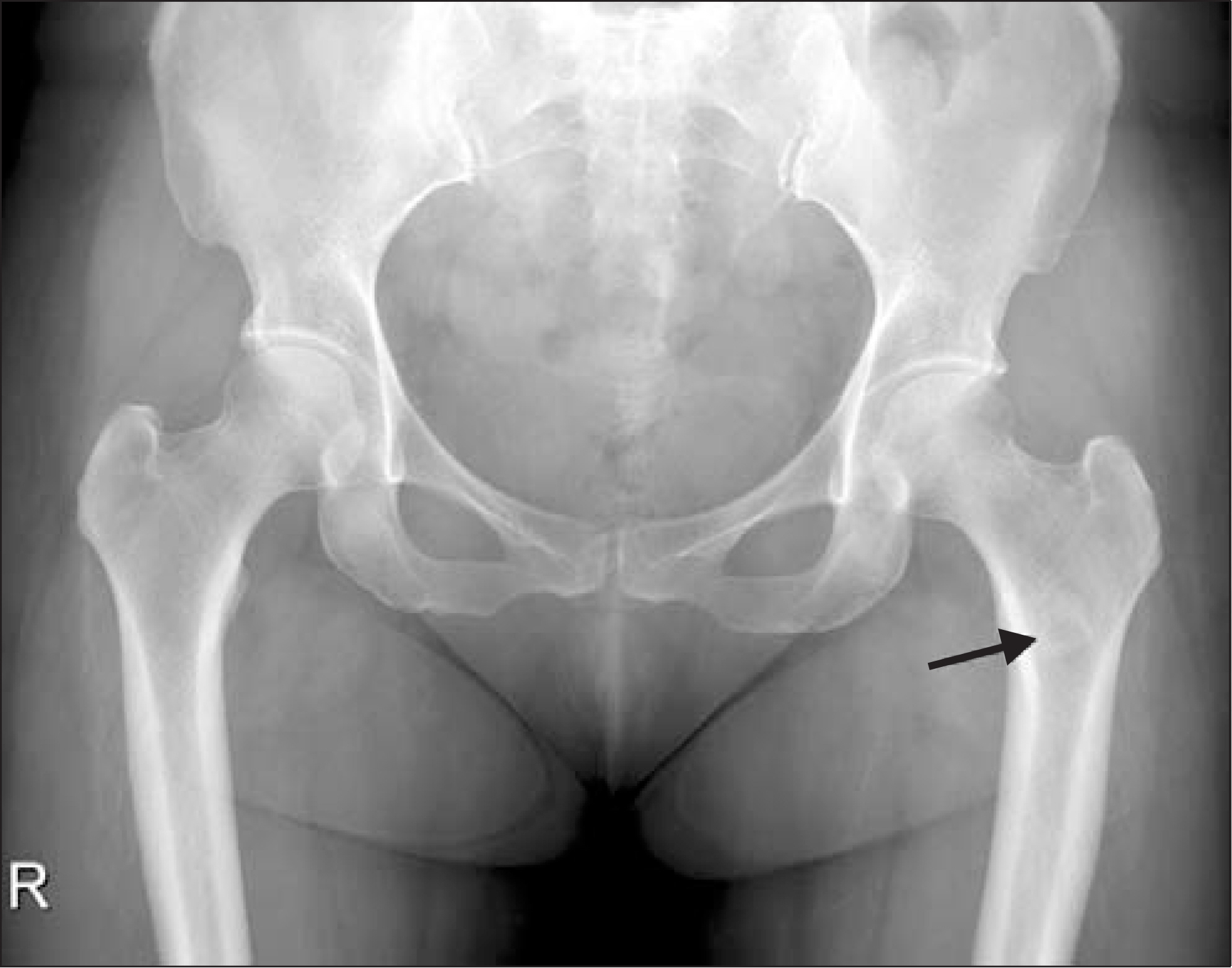
Figure 2. Radiograph in a 46-year-old woman shows an intramedullary lesion with a diffuse sclerotic lesion (arrow) on left proximal femur.

Figure 3. A 46-year-old woman who underwent MRI for intermittent left hip pain after radiation for one month. Left proximal femoral lesion was interpreted as a fibrous dysplasia based on MR findings. T1-weighted (A) and T2-weighted (B) coronal images show a well-defined hypointense lesion (arrows in A and B) in left proximal femur. Fat-suppressed T2-weighted coronal image (C) shows moderate perilesional hyperintense signal (arrowheads) on the left proximal femur suggesting post-radiation edema. Contrast-enhanced T1-weighted coronal image (D) shows mild contrast enhancement in the mass (arrow). Axial fat-suppressed contrast-enhanced T1-weighted image (E) also shows mild contrast enhancement in the mass. Adjacent muscles in the medial compartment of the thigh shows relatively well-demarcated contrast enhancement, suggesting post-radiation edema.
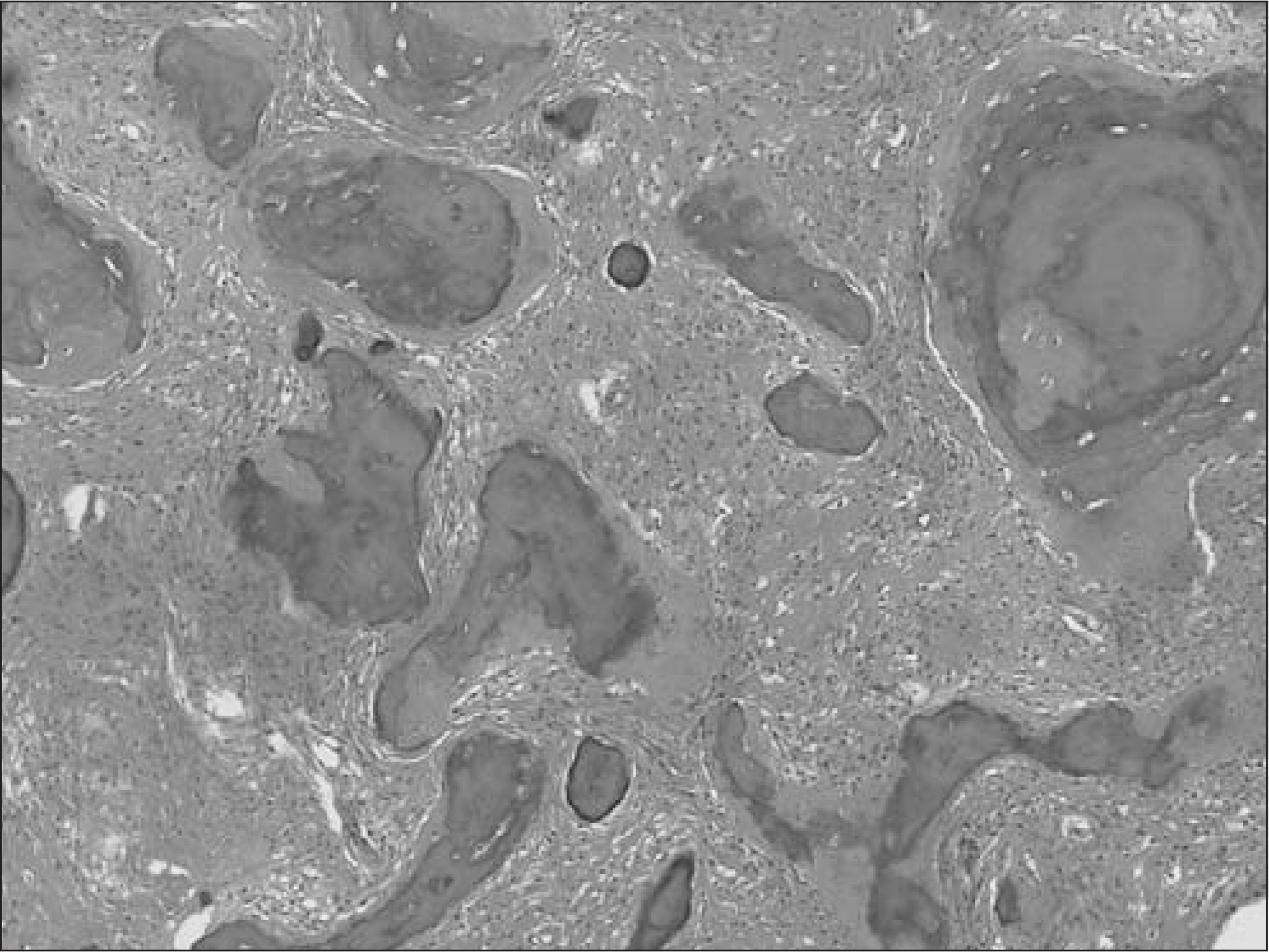
Figure 4. In microscopic examination, fibrous tissue blended into the bone spicules, which had irregular shapes and imperceptible osteoblast rimming (H&E ×100).
Reference
-
1. Kao CH, Sun SS, Shen YY, Chen YK. Misdiagnosis of multiple bone metastases due to increased FDG uptake in polyostotic fibrous dysplasia. Clin Nucl Med. 2007; 32:409–10.
Article2. Stegger L, Juergens KU, Kliesch S, Wormanns D, Weckesser M. Unexpected finding of elevated glucose uptake in fibrous dysplasia mimicking malignancy: contradicting metabolism and morphology in combined PET/CT. Eur Radiol. 2007; 17:1784–6.
Article3. Strobel K, Bode B, Lardinois D, Exner U. PET-positive fibrous dysplasia–a potentially misleading incidental finding in a patient with intimal sarcoma of the pulmonary artery. Skeletal Radiol. 2007; 36(Suppl 1):24–8.4. Shigesawa T, Sugawara Y, Shinohara I, Fujii T, Mochizuki T, Morishige I. Bone metastasis detected by FDG PET in a patient with breast cancer and fibrous dysplasia. Clin Nucl Med. 2005; 30:571–3.
Article5. Tsuyuguchi N, Ohata K, Morino M, et al. Magnetic resonance imaging and [11C]methyl-L-methionine positron emission tomography of fibrous dysplasia–two case reports. Neurol Med Chir (Tokyo). 2002; 42:341–5.6. Cook GJ, Houston S, Rubens R, Maisey MN, Fogelman I. Detection of bone metastases in breast cancer by 18F-FDG PET: differing metabolic activity in osteoblastic and osteolytic lesions. J Clin Oncol. 1998; 16:3375–9.7. Jee WH, Choi KH, Choe BY, Park JM, Shinn KS. Fibrous dysplasia: MR imaging characteristics with radiopathologic correlation. Am J Roentgenol. 1996; 167:1523–7.
Article8. Maeda M, Kimura H, Tsuchida C, Ishii Y, Kubota T. MR imaging of monostotic fibrous dysplasia of the clivus. A case report. Acta Radiol. 1993; 34:527–8.9. Utz JA, Kransdorf MJ, Jelinek JS, Moser RP Jr, Berrey BH. MR appearance of fibrous dysplasia. J Comput Assist Tomogr. 1989; 13:845–51.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Fibrous Dysplasia Mimicking Bone Metastasis on Both Bone Scintigraphy and 18F-FDG PET-CT: Diagnostic Dilemma in a Patient with Breast Cancer
- Contralateral Internal Mammary Lymphadenopathy Mimicking Metastasis in a Patient with a History of Breast Cancer and Prior Interstitial Mammoplasty by Paraffin Injection: MRI, PET-CT, and Pathological Findings
- COVID-19 Vaccine-Related Axillary and Cervical Lymphadenopathy in Patients with Current or Prior Breast Cancer and Other Malignancies: Cross-Sectional Imaging Findings on MRI, CT, and PET-CT
- Polyostotic Fibrous Dysplasia Mimicking Multiple Bone Metastases in a Patient with Ductal Carcinoma In Situ
- Solitary Plasmacytoma of the Sternum Mimicking Bone Metastasis in a Patient with a History of Breast Cancer Evaluated by F-18-FDG PET/CT
