Secondary Chondrosarcoma Arising from Osteochondroma(tosis)
- Affiliations
-
- 1Department of The Musculoskeletal Oncology Group, School of Medicine, Catholic University, Uijeongbu, Korea. wjbahk@catholic.ac.kr
- KMID: 2006338
- DOI: http://doi.org/10.5292/jkbjts.2010.16.1.21
Abstract
- PURPOSE
To analyze clinical, radiological and pathological features as well as clinical outcome after surgical treatment of patients with secondary chondrosarcoma arising from osteochondroma(tosis).
MATERIALS AND METHODS
We retrospectively reviewed clinical records, radiographs, pathologic slides of 14 patients. Nine patients were male and five were female. The mean age was 34 years. The mean follow-up period was 54 months.
RESULTS
All patients had a history of previous mass since childhood or puberty. Preexisted osteochondroma was single in 3 patients and multiple in 10. Remaining 1 patient had multiple osteochondromatosis with enchondromatosis. MRI clearly provided thickness of cartilage cap, which was over 2 cm except in 2 cases. Chondrosarcoma was grade 1 in all except 1 case, which was grade 2. Wide excision was performed in 10 patients, marginal excision in 3 and amputation in 1. Twelve patients were doing very well without evidence of disease. Among 3 patients with marginal excision, 1 patient had local recurrence and 1 patient died of disease.
CONCLUSION
Comprehensive understanding of clinical, radiological and pathological features of secondary chondrosarcoma is warranted for accurate diagnosis. The best result can be expected with early recognition of malignant change of osteohcondroma(tosis) and wide excision.
MeSH Terms
Figure
-

Figure 1. Plain radiograph shows irregularity of the surface and radiolucency with punctuated calcification in right inferior ramus.

Figure 2. CT scan reveals well-defined bony mass with indistinctive sclerotic margin and punctuated calcification within the mass.

Figure 3. Gross finding shows cartilage cap with maximum 2.8 cm of thickness.

Figure 4. Plain radiograph demonstrates a huge soft tissue mass with indistinctive margin and scattered punctuated calcification within the mass in left pelvic area.
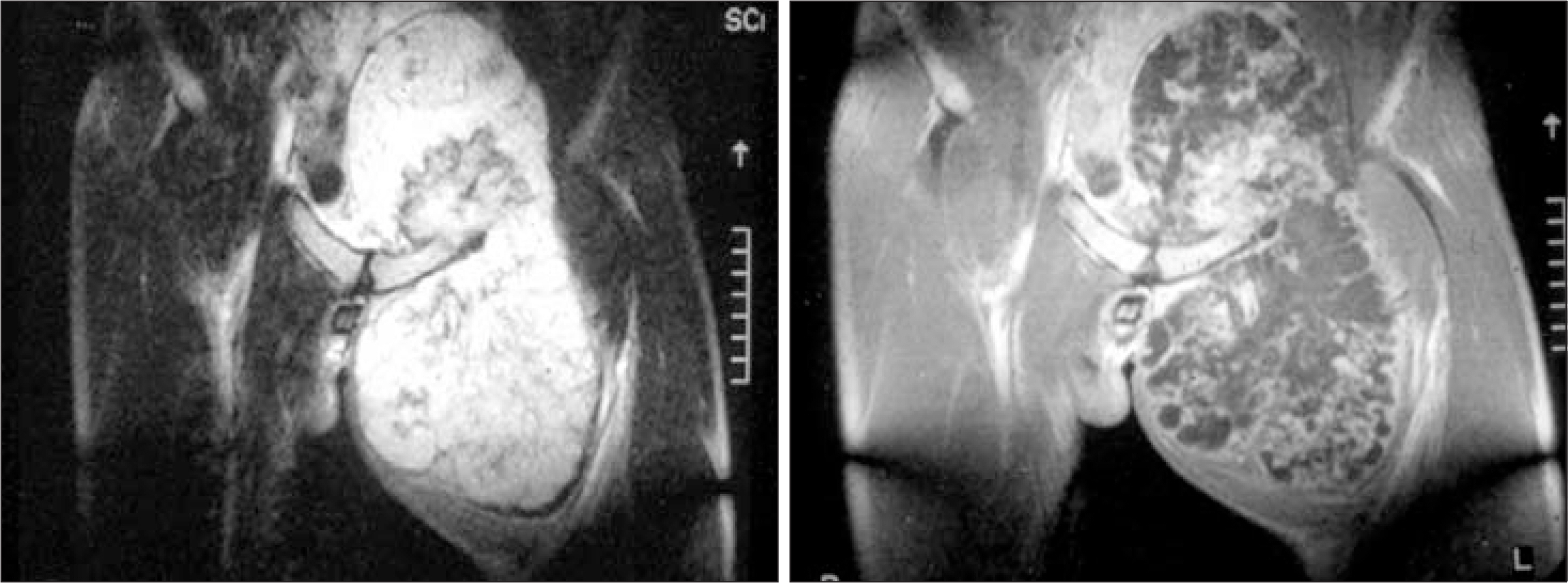
Figure 5. MRI shows a large inhomogeneous, irregularly marginated mass with maximum 4 cm-thick cartilage cap of decreased T1 and increased T2 signal intensities.
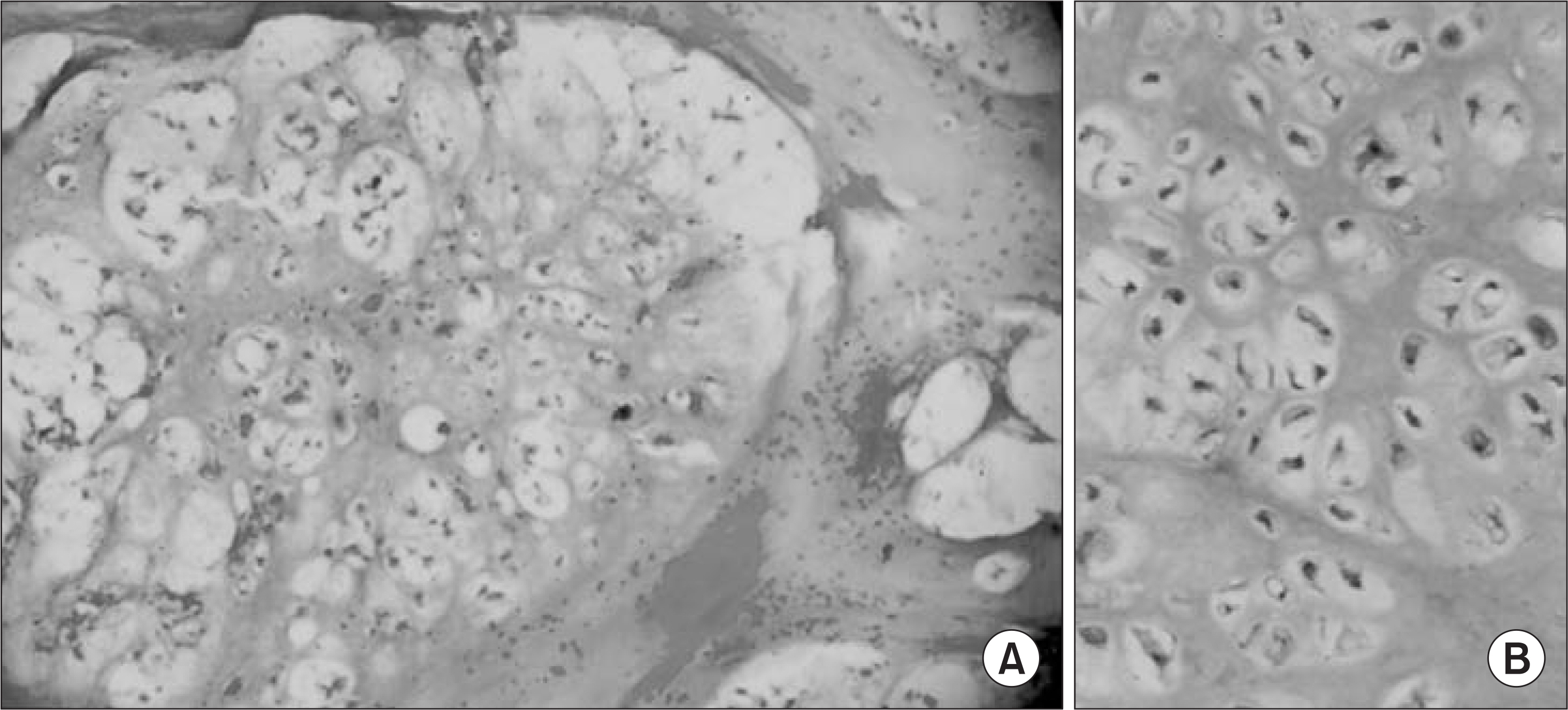
Figure 6. (A) Low-power microscopic examination shows high cellularity (H&E, ×40). (B) High-power examination reveals atypism with hyperchromatic neclei and a few binucelated chondrocytes (H&E, ×200).
Reference
-
1. Ahmed AR, Tan TS, Unni KK, Collins MS, Wenger DE, Sim FH. Secondary chondrosarcoma in osteochnodroma: Report of 107 patients. Clin Orthop Relat Res. 2003; 411:193–206.2. Garrision RC, Unni KK, McLeod RA, Pritchard DJ, Dahlin DC. Chondrosarcoma arising in ostechondroma. Cancer. 1982; 49:1890–7.3. Nojima T, Yamashiro K, Fujita M, Isu K, Ubayama Y, Yama-waki S. A case of osteosarcoma arising in a solitary osteochondroma. Acta Orthop Scand. 1991; 62:290–2.
Article4. Wuisman PI, Jutte PC, Ozaki T. Secondary chondrosarcoma in osteochondromas. Medullary extension in 15 of 45 cases. Acta Orthop Scand. 1997; 68:396–400.
Article5. Barnes R, Catto M. Chnodrosarcoma of bone. J Bone Joint Surg. 1966; 48:729–64.6. Hong KD, Ha SS, Park YK, Lee HJ, Cha HJ. Chondrosarcoma of the Calcaneus in 13 year old Aged Patient- A Case Report -. J Korean Bone Joint Tumor Soc. 2001; 7:59–63.7. Campanacci M. Peripheral chondrosarcoma. Campanacci M, editor. Bone and soft tissue tumors. 2nd ed.New York: Springer;1999. p. 335–61.
Article8. Murphey MD, Choi JJ, Kransdorf MJ, Flemming DJ, Gannon FH. Imaging of osteochondroma: variants and complications with radiologic-pathologic correlation. Radiographics. 2000; 20:1407–34.
Article9. Peterson HA. Multiple hereditary osteochondromata. Clin Orthop. 1989; 239:222–30.
Article10. Mirra JM. Malignant Cartilaginous Exostoses. Mirra JM, editor. Bone tumors: Clinical, Radiologic, and pathologic Correlations. Vol 2. Philadelphia: Lea & Febiger;1989. p. 1660–73.11. O'neal LW, Ackerman LV. Chondrosarcoma of bone. Cancer. 1952; 5:551–77.12. Norman A, Sissons HA. Radiographic hallmarks of peripheral chondrosarcoma. Radiology. 1984; 151:589–96.
Article13. Bernard SA, Murphey MD, Flemming DJ, Kransdorf MJ. Improved differentiation of benign osteochondromas from secondary chondrosarcomas with standardized measurement of cartilage cap at CT and MR imaging. Radiology. 2010; 255:857–65.
Article14. Pritchard DJ, Lunke RJ, Taylor WF, Dahlin DC, Medley BE. Chondrosarcoma: A clinicopathologic and statistical analysis. Cancer. 1980; 45:149–57.
Article15. Dahlin DC, Henderson ED. Chondrosarcoma, a surgical and pathological problem: Review of 212 cases. J Bone Joint Surg. 1956; 38:1025–38.16. Evans HL, Ayala AG, Romsdahl MM. Prognostic factors in chondrosarcoma of bone: A clinicopathologic analysis with emphasis on histologic grading. Cancer. 1977; 40:818–31.17. Gitels S, Bertoni F, Picci P, Campanacci M. Chondrosarcoma of bone: The experience at the Istituto Ortopedico Rizzoli. J Bone Joint Surg. 1981; 63:1248–57.18. Solomon L. Chondrosarcoma in hereditary multiple exostosis. S Afr Med J. 1974; 48:671–6.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Secondary Chondrosarcoma from an Osteochondroma of the Proximal Tibia Involving the Fibula
- Osteosarcoma Arising in a Multiple Osteochondromatosis A Case Report -
- A Case of Intraarticular Osteochondroma Arising from Patella
- Chondrosarcoma Arising from Benign Bone Tumor due to Malignant Transformation
- Clear Cell Chondrosarcoma Arising in Hyoid Bone
