Congenital Anomalies of the Coronary Sinus: A Pictorial Essay
- Affiliations
-
- 1Department of Radiology, College of Medicine, Kyung Hee University, Seoul, Korea. kwon98@khu.ac.kr
- KMID: 2002887
- DOI: http://doi.org/10.3348/jksr.2013.69.1.29
Abstract
- Congenital anomalies involving the coronary sinus (CS) tend to receive relatively little attention because they rarely cause clinical symptoms or disturbances of cardiac function. However, as imaging modalities have been developed over time, the detailed anatomy of the heart, including CS anomalies, can now be evaluated more precisely. The purpose of this pictorial review is to illustrate multi-detector computed tomography findings of various congenital anomalies of the CS. The cardiac venous system and its embryologic development are also described in detail to familiarize radiologists with various congenital anomalies of the CS.
MeSH Terms
Figure
-
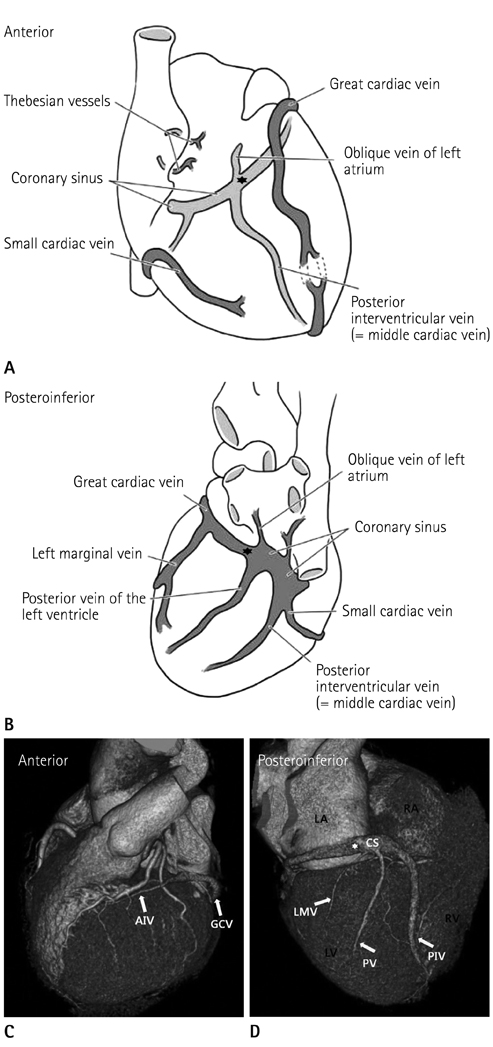
Fig. 1 Venous drainage of the heart. Anterior (A, C) and posteroinferior (B, D) views of the heart. The coronary sinus (CS) runs along the inferior aspect of the heart in the atrioventricular groove before emptying into the right atrium (RA). The posterior interventricular vein (PIV) courses in the posterior interventricular groove from the base to the apex. The posterior vein (PV) of the left ventricle and the left marginal vein (LMV) are the next main branches. The great cardiac vein (GCV) courses in the left atrioventricular groove with the left circumflex artery. The anterior interventricular vein (AIV) continues in the anterior interventricular groove, adjacent to the left anterior descending artery. Note.-★= valve of Vieussens (junction between CS and GCV), LA = left atrium, LV = left ventricle, RV = right ventricle
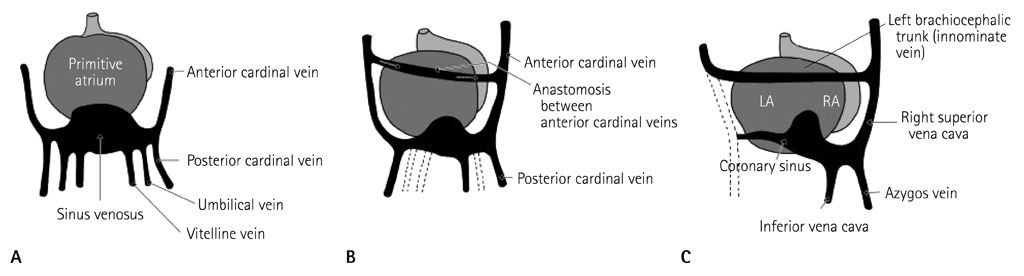
Fig. 2 Development of the cardiac veins. Posterior view of the heart of an embryo at four weeks (A), eight weeks (B), and ten weeks (C). By the eighth week, the umbilical veins and the left vitelline vein regress. The left and right anterior cardinal veins connect through a vessel that becomes the left brachiocephalic vein. The right horn of the sinus venosus becomes the posterior wall of the right atrium, and the cardinal veins become the vena cava. The left common cardinal vein is occluded, and the left horn of the sinus venosus forms the coronary sinus and the oblique vein of the left atrium (vein of Marshall). Adapted from Moore KL, Persaud TVN. The developing human: clinically oriented embryology, 7th ed (8). Note.-LA = left atrium, RA = right atrium
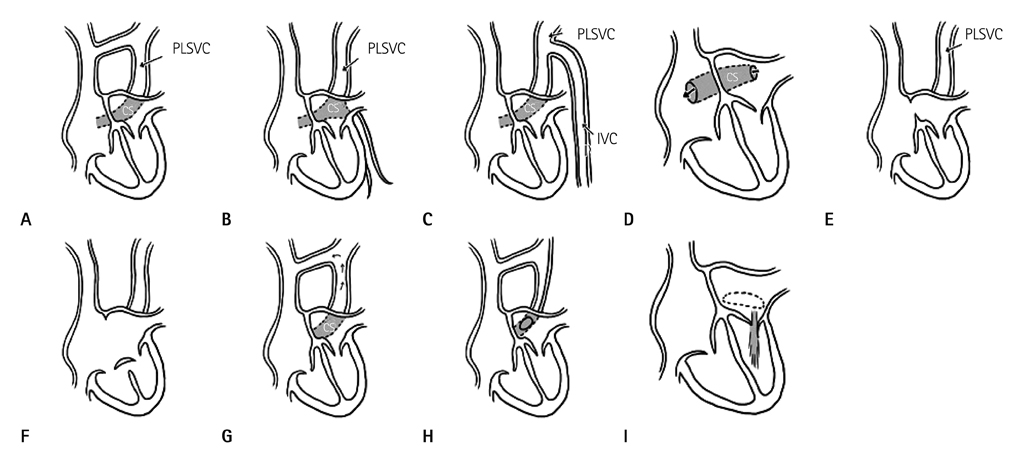
Fig. 3 Illustrations of congenital anomalies of the coronary sinus (CS). Enlargement of the CS associated with (A) persistent left superior vena cava (PLSVC), (B) partial anomalous hepatic venous connection, (C) continuity of the inferior vena cava with PLSVC through the hemiazygos vein, and (D) the absence of the CS roof (unroofed CS). The absence of the CS associated with (E) PLSVC and atrial septal defect. (F) PLSVC and a variety of persistent common atrioventricular canals. The atrial septal defect involves the entire lowermost portion. Atresia of the right atrial ostium of the CS associated with (G) functional PLSVC, with blood returning in a retrograde direction into the right atrium through the left innominate vein; (H) a narrow PLSVC joins an anomalous CS that communicates with the left atrium; and (I) multiple communications between CS and related atria. Adapted from Mantini E, Grondin CM, Lillehei CW, Edwards JE. Circulation 1966;33:317-327 (5).
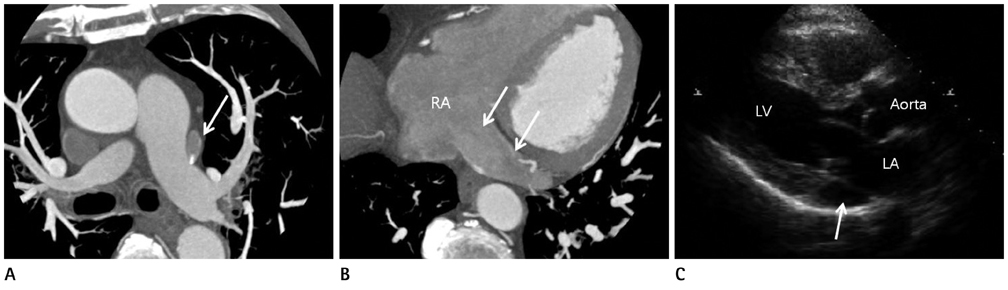
Fig. 4 Incidentally found persistent left superior vena cava (PLSVC) with a dilated coronary sinus (CS) in a 49-year-old female. A. Axial CT MIP image showing that the PLSVC (arrow) lies lateral to the left main pulmonary artery. The right superior vena cava is noted in its normal position. B. The dilated CS (arrows) drains into the right atrium (RA). C. The parasternal long axis view in transthoracic echocardiography showing an abnormally dilated coronary sinus (arrow). Note.-LA = left atrium, LV = left ventricle, MIP = maximum intensity projection
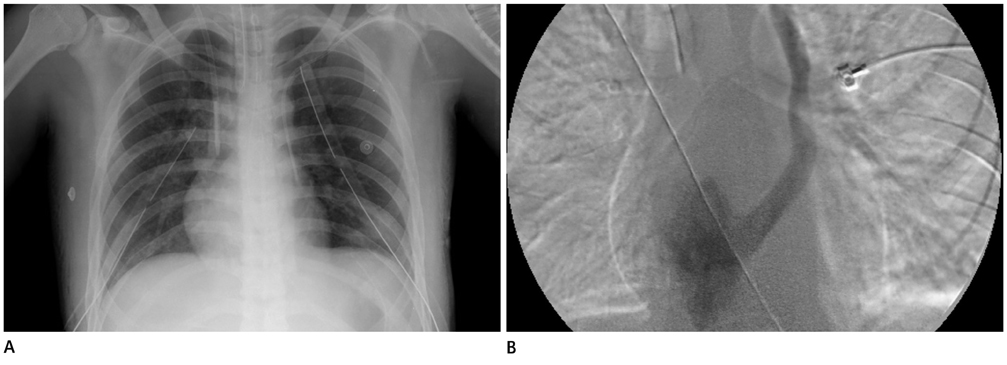
Fig. 5 Incidentally found persistent left superior vena cava (PLSVC) in a 17-year-old boy who underwent both central venous catheter and chest tube insertion due to a traffic accident. A. Plain chest radiograph showing the hemodialysis catheter in the right superior vena cava and the subclavian catheter in the PLSVC. B. Left superior venacavogram confirming that the persistent left superior vena cava drains through the coronary sinus into the right atrium.
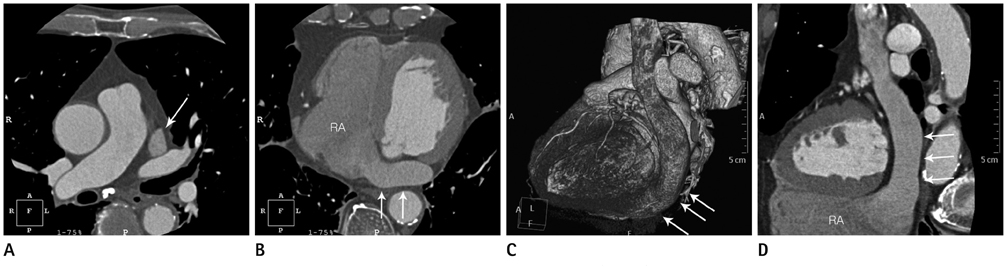
Fig. 6 Absence of the right superior vena cava with persistent left superior vena cava (PLSVC). A. Axial CT image showing the PLSVC (arrow) without the right superior vena cava. B. The severely dilated coronary sinus (CS) (arrows) drains into the right atrium (RA). C, D. 3D VR image (C) and curved MPR image (D) showing the PLSVC draining into the severely dilated CS (arrows) inferior to the left atrioventricular groove. Note.-3D VR = three dimensional volume rendering

Fig. 7 Incidental unusual communication of the severely dilated great cardiac vein with the left atrium and a partially unroofed coronary sinus (CS) in a 69-year-old female. A. Axial CT MIP images demonstrate a severely dilated great cardiac vein (white arrow) having a communication with the left atrium just below the left superior pulmonary vein level. B. The coronary sinus (white arrows) is also dilated and drains into the right atrium. C. Curved MPR image showing an abnormal communication of the coronary sinus with the left atrium (white arrows). The partially unroofed coronary sinus can be seen (black arrow). Note.-MIP = maximum intensity projection, MPR = multiplanar reconstruction, RA = right atrium, LA = left atrium
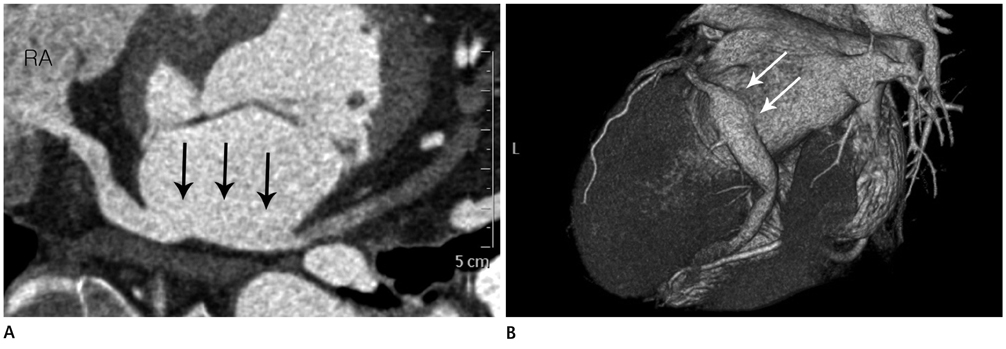
Fig. 8 Incidentally found partially unroofed coronary sinus (CS) in a 65-year-old woman. A. Curved MPR image showing a partially unroofed CS, the site of unroofing (arrows), and dense contrast (left-to-right shunt) entering the right atrium (RA). B. 3D VR image showing a partial direct communication (arrows) between the CS and the left atrium and mild dilatation of the CS. Note.-MPR = multiplanar reconstruction, 3D VR = three dimensional volume rendering

Fig. 9 A case of coronary sinus (CS) orifice atresia with a persistent left superior vena cava (PLSVC) and an aberrant communicating vein into the right atrium in a 48-year-old male. (A) Left lateral view of the 3D VR image showing the PLSVC communicating with a mildly dilated CS. 3D VR images (B, C) and curved MPR image (D) showing the CS terminating as a blind sac without any grossly visible communication with the right atrium (RA). There is also an unusual exit (arrows) from the CS through the posterior interventricular vein that runs into the right ventricular and atrial wall. This unusual vein communicates with the RA cavity via a small orifice. Note.-LA = left atrium, MPR = multiplanar reconstruction, RV = right ventricle, 3D VR = three dimensional volume rendering
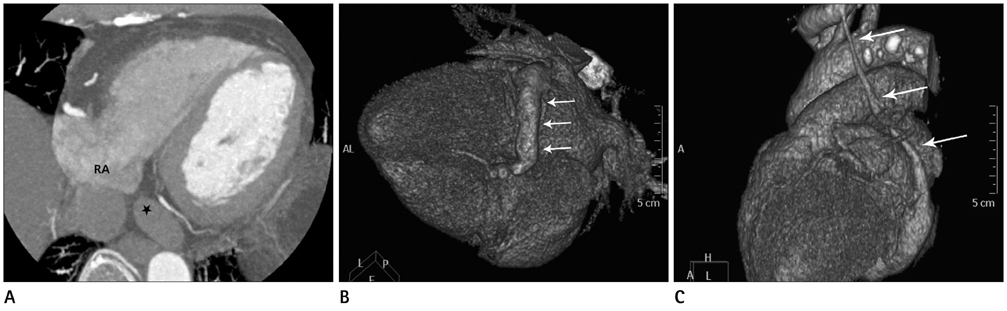
Fig. 10 Coronary sinus (CS) orifice atresia with persistent left superior vena cava (PLSVC) in a 73-year-old female. A. Axial CT MIP image showing a blind ostium (star) of the CS to the right atrium. B, C. 3D VR images showing (B) a dilated CS (arrows) and (C) the PLSVC (arrows) communicating with the dilated CS. Note.-MIP = maximum intensity projection, 3D VR = three dimensional volume rendering
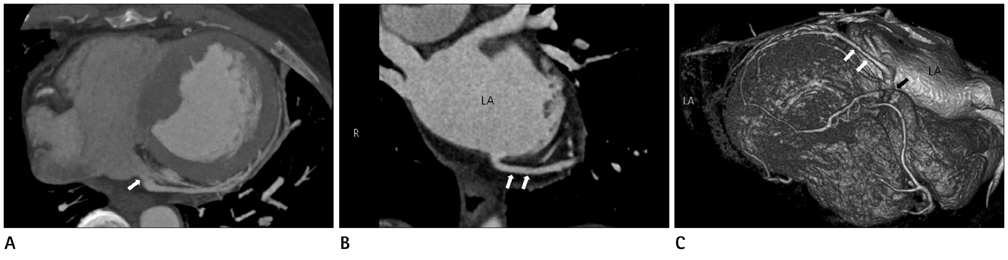
Fig. 11 Coronary sinus (CS) orifice stenosis with aberrant coronary venous drainage into the left atrium (LA) in a 59-year-old female. CT MIP images showing (A) the CS orifice stenosis (white arrow) and (B) aberrant coronary venous drainage (white arrows) into the LA. 3D VR image (C) also showing the CS orifice stenosis (black arrow) and aberrant coronary venous drainage into the LA (white arrows). Note.-MIP = maximum intensity projection, 3D VR = three dimensional volume rendering
Reference
-
1. Saremi F, Muresian H, Sánchez-Quintana D. Coronary veins: comprehensive CT-anatomic classification and review of variants and clinical implications. Radiographics. 2012; 32:E1–E32.2. Muster AJ, Naheed ZJ, Backer CL, Mavroudis C. Is surgical ligation of an accessory left superior vena cava always safe? Pediatr Cardiol. 1998; 19:352–354.3. Ruengsakulrach P, Buxton BF. Anatomic and hemodynamic considerations influencing the efficiency of retrograde cardioplegia. Ann Thorac Surg. 2001; 71:1389–1395.4. Chou MC, Wu MT, Chen CH, Lee MH, Tzeng WS. Multidetector CT findings of a congenital coronary sinus anomaly: a report of two cases. Korean J Radiol. 2008; 9:Suppl. S1–S6.5. Mantini E, Grondin CM, Lillehei CW, Edwards JE. Congenital anomalies involving the coronary sinus. Circulation. 1966; 33:317–327.6. O'Brien JP, Srichai MB, Hecht EM, Kim DC, Jacobs JE. Anatomy of the heart at multidetector CT: what the radiologist needs to know. Radiographics. 2007; 27:1569–1582.7. Bax JJ, Abraham T, Barold SS, Breithardt OA, Fung JW, Garrigue S, et al. Cardiac resynchronization therapy: Part 2--issues during and after device implantation and unresolved questions. J Am Coll Cardiol. 2005; 46:2168–2182.8. Moore KL, Persaud TVN. The developing human: clinically oriented embryology. 7th ed. Philadelphia, PA: Saunders;2003. p. xv. p. 560.9. Anderson RH, Brown NA, Moorman AF. Development and structures of the venous pole of the heart. Dev Dyn. 2006; 235:2–9.10. Cha EM, Khoury GH. Persistent left superior vena cava. Radiologic and clinical significance. Radiology. 1972; 103:375–381.11. Pálinkás A, Nagy E, Forster T, Morvai Z, Nagy E, Varga A. A case of absent right and persistent left superior vena cava. Cardiovasc Ultrasound. 2006; 4:6.12. Edwards JE, DuShane JW, Alcott DL, Burchell HB. Thoracic venous anomalies. III. Atresia of the common pulmonary vein, the pulmonary veins draining wholly into the superior vena cava. AMA Arch Pathol. 1951; 51:446–460.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Congenital Anomalies of the Coronary Arteries
- Anomalous Right Coronary Artery From the Left Coronary Sinus With an Interarterial Course: Is It Really Dangerous?
- Anomalous Origin of the Left Coronary Artery from the Right Sinus of Valsalva, which Presented as Acute Myocardial Infarction
- Multidetector CT Findings of a Congenital Coronary Sinus Anomaly: a Report of Two Cases
- Sudden Death Associated with Anomalous Left Coronary Artery Origin from Right Sinus of Valsalva with Posterior Course
