Multidetector CT Findings of a Congenital Coronary Sinus Anomaly: a Report of Two Cases
- Affiliations
-
- 1Department of Radiology, Yong-Kang Campus, Chi-Mei Medical Center, Taiwan, R.O.C. meichuntw@yahoo.com
- 2Section of Thoracic and Circulation Imaging, Department of Radiology, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan, R.O.C.
- 3Faculty of medicine, School of medicine, National Yang Ming University, Taipei, Taiwan, R.O.C.
- 4Department of Radiology, National Defense Medical Center, Taiwan, R.O.C.
- 5Department of Radiological Technology, Central Taiwan University of Science and Technology, Taichung, Taiwan, R.O.C.
- KMID: 1100093
- DOI: http://doi.org/10.3348/kjr.2008.9.s.s1
Abstract
- Congenital coronary sinus anomalies are extremely rare, and they have received relatively little attention. This is probably due to the lack of both clinical symptoms and significant cardiac functional disturbance. We present two cases of a coronary sinus anomaly and briefly review the literature. Recognizing and being familiar with the variations of a congenital coronary sinus anomaly in congenital heart disease may avoid a misinterpretation of cardiac catheterization findings and the troublesome disruption of coronary sinus blood return during the surgical management of cardiac lesions.
Keyword
MeSH Terms
Figure
-

Fig. 1 Congenital coronary sinus anomaly in 60-year-old woman with Ebstein's anomaly. A, B. Dorsal view of reconstructed volume-rendered image (A) and maximum-intensity-projection image (B) reveal normal coronary sinus (arrow) drain into right atrium (RA). RA = right atrium; LA = left atrium C. Dorsal view of reconstructed volume-rendered image reveals abnormal engorged coronary sinus (long white arrow) without gross communication with right atrium (RA). There was small tortuous vascular channel (short black arrow) drain into left atrium (LA). Atrialization portion of right ventricle also could be identified (black star). D. Series maximum-intensity-projection images confirmed that there was no communication between abnormally engorged coronary sinus (long white arrows) and right atrium (RA). In addition, there was small tortuous vascular channel with high contrast density (black arrows) located between engorged coronary sinus and right atrium (RA). Small foci of high contrast density within coronary sinus also had been found (black arrows). E. Post-processing oblique-dorsal view of reconstructed volume-rendered image with total removal of right atrium revealed that this small tortuous vascular channel (black arrows) connected coronary sinus (CS) and left atrium (LA). RA = right atrium; LA = left atrium; CS = coronary sinus
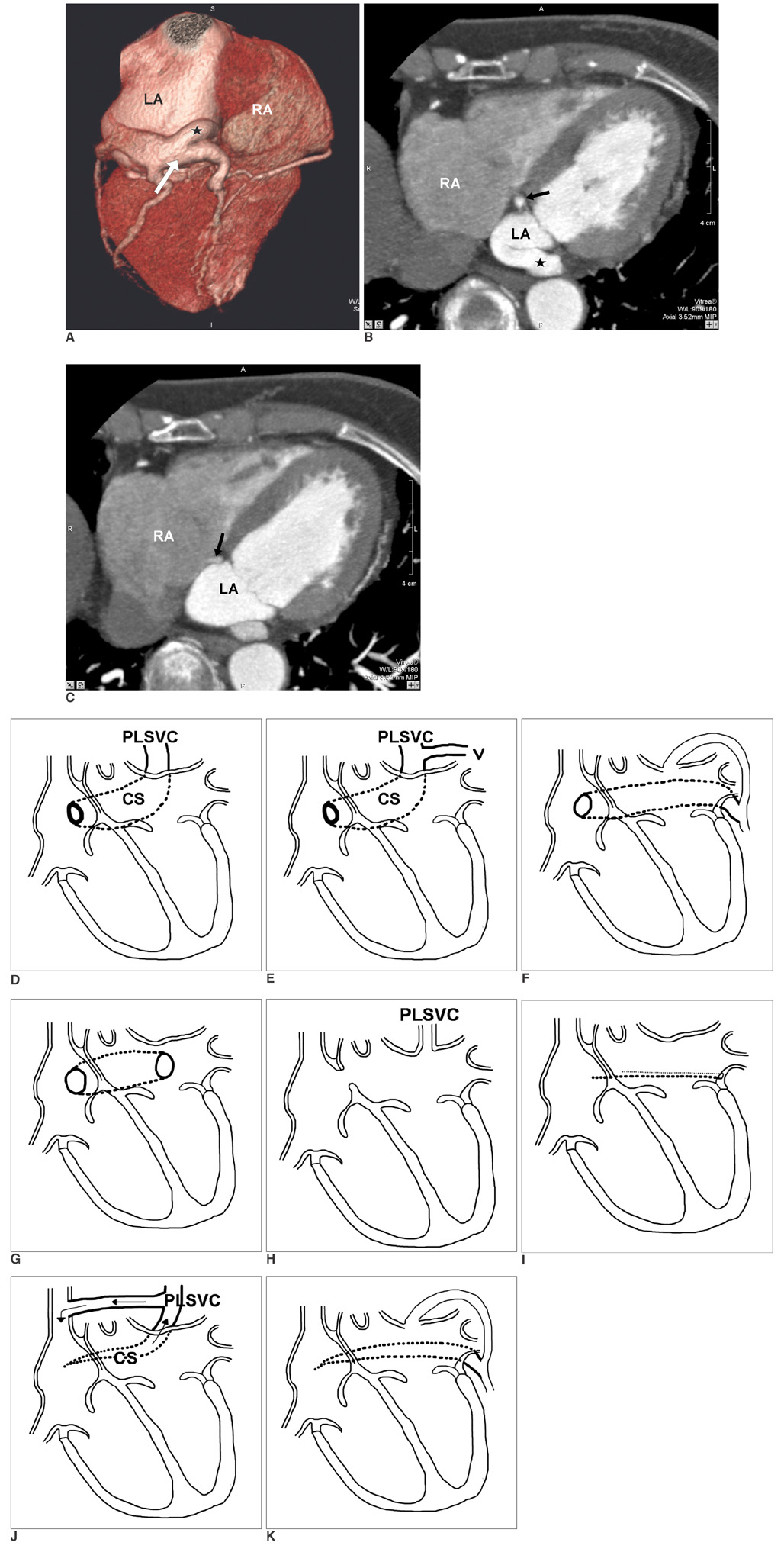
Fig. 2 Coronary sinus anomaly with stenosis of right atrial ostium and coexisting levoatriocardinal vein communication to left atrium in 64-year-old woman. A. Dorsal view of reconstructed volume-rendered image reveals abnormal engorged coronary sinus (long white arrow) without grossly visible communication with right atrium (RA). There was engorged vascular channel (black star) arising from coronary sinus that was highly suggestive of communication with left atrium (LA). B. Maximum-intensity-projection image revealed that aforementioned vascular channel (black star) was connected to left atrium (LA) with large opening. Evidence of large left-to-right shunting is also noted according to equal high-contrast density within CS and LA. Stenostic end of coronary sinus into right atrium (RA) was also seen (black arrow). C. Sequential maximum-intensity-projection image next to B demonstrates stenostic right atrial ostium (black arrow) of coronary sinus. RA = right atrium, LA = left atrium D-G. Illustration of enlargement of coronary sinus (CS) associated with (D) a persistent left superior vena cava (PLSVC); (E) PLSVC and other anomalous systemic venous return; (F) anomalous left-to-right shunt from left atrium; (G) unusually large communication between left atrium and coronary sinus (modified from Mantini and colleagues (1)). H. Illustration of absence of coronary sinus, which is always associated with persistent left superior vena cava (PLSVC) and atrial septal defect (modified from Mantini and colleagues (1)). I. Illustration of hypoplasic coronary sinus; cardiac veins failed to join coronary sinus and emptied into atrial chamber through dilated thebesian channels (modified from Mantini and colleagues (1)). J. With functional persistent left superior vena cava (PLSVC), blood returns in retrograde direction, passing upward to persistent left superior vena cava (PLSVC), left innominate vein, right superior vena cava, and eventually into right atrium. K. Without persistent left superior vena cava (PLSVC), blood returns through levoatriocardinal vein then into left atrium (modified from Mantini and colleagues (1)).
Reference
-
1. Mantini E, Grondin CM, Lillehei CW, Edwards JE. Congenital anomalies involving the coronary sinus. Circulation. 1966. 33:317–327.2. Ruengsakulrach P, Buxton BF. Anatomic and hemodynamic considerations influencing the efficiency of retrograde cardioplegia. Ann Thorac Surg. 2001. 71:1389–1395.3. Jha NK, Gogna A, Tan TH, Wong KY, Shankar S. Atresia of coronary sinus ostium with retrograde drainage via persistent left superior vena cava. Ann Thorac Surg. 2003. 76:2091–2092.4. Rose AG, Beckman CB, Edwards JE. Communication between coronary sinus and left atrium. Br Heart J. 1974. 36:182–185.5. Miraldi F, di Gioia CR, Proietti P, De Santis M, d'Amati G, Gallo P. Cardinal vein isomerism: an embryological hypothesis to explain a persistent left superior vena cava draining into the roof of the left atrium in the absence of coronary sinus and atrial septal defect. Cardiovasc Pathol. 2002. 11:149–152.6. Neuser H, Kerber S, Schumacher B. Images in cardiovascular medicine. Fistulous communication between coronary sinus and left atrium. Circulation. 2002. 106:E137–E138.7. Edwards JE, DuShane JW. Thoracic venous anomalies. Arch Pathol. 1950. 49:517–537.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Erratum
- A Single Coronary Artery with the Right Coronary Artery Originating from the Left Anterior Descending Artery Detected by Cardiac CT: A Case Report
- Acute Myocardial Infarction in Patients With Single Coronary Artery: A Case Report
- Anomalous Origin of the Left Circumflex Coronary Artery from the Right Sinus of Valsalva Identified by Imaging with Multidetector Computed Tomography
- Congenital Anomalies of the Coronary Sinus: A Pictorial Essay
