Anomalous Right Coronary Artery From the Left Coronary Sinus With an Interarterial Course: Is It Really Dangerous?
- Affiliations
-
- 1Department of Radiology, St. Paul's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea. leebae@catholic.ac.kr
- KMID: 1826015
- DOI: http://doi.org/10.4070/kcj.2009.39.5.175
Abstract
- Anomalous origin of the right or left coronary artery from the contralateral sinus of Valsalva is often asymptomatic, but many patients, particularly young ones, present with sudden death or myocardial ischemia without symptoms. The mechanism of sudden death in this entity is unclear and has not been fully evaluated. These anomalies are rare, and many cardiologists and radiologists are unfamiliar with them. Surgical repair is recommended, especially with anomalous origin of the left coronary artery (LCA). However, there is controversy concerning the treatment of anomalous right coronary artery (RCA) with interarterial course due to its relatively high incidence and the fact that it leads to few, if any, clinical problems.
MeSH Terms
Figure
-
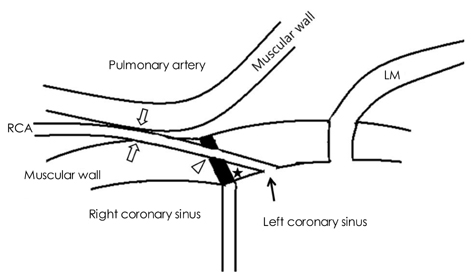
Fig. 1 Possible mechanisms of coronary flow restriction of the anomalous right coronary artery (RCA) from the left coronary sinus with interarterial course. The intramural course of the anomalous RCA is long, and the takeoff angle of the RCA orifice is acute (★) compared with that of the normal left main coronary artery (LM). A combined slit-like orifice (arrow) is also seen. If the anomalous RCA passes through the aortic commissure (black column), compression by the aortic commissure (open arrow head) is also possible. Compression of the anomalous RCA by the pulmonary artery and aorta (open arrows) is also feasible.

Fig. 2 A 68-year-old man presented with intermittent chest pain. Oblique axial MPR imaging (A) shows luminal narrowing at the takeoff portion of the anomalous RCA (arrow), but the oblique sagittal MPR (B) image shows a normal-sized anomalous RCA (arrow). Oblique coronal MPR imaging (C) shows an interarterial course; the lumen of the anomalous RCA is ovoid (arrow). This patient required no treatment. MPR: multiplanar reconstruction, RCA: right coronary artery, PA: pulmonary artery, Ao: aorta, LCC: left coronary sinus, RCC: right coronary sinus.
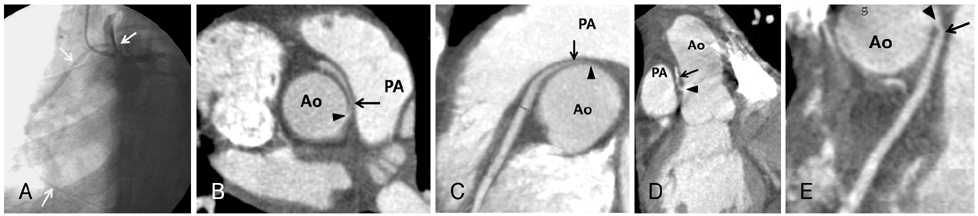
Fig. 3 A 39-year-old woman presented with persistent chest pain and palpitations. Angiography (A) showed an anomalous RCA (arrow) originating from the left coronary sinus, but selective cannulation failed due to the small orifice and angulation. Preoperative oblique axial (B) and curved (C) MPR images showed severe luminal narrowing (arrow) of the proximal portion of the anomalous RCA, as well as a small orifice (arrow head) with acute angle takeoff. After an unroofing procedure was performed, postoperative oblique (D) and curved (E) MPR images showed a more distended proximal anomalous RCA (arrow) and orifice (arrow head) with increased takeoff angle. The unroofing procedure manipulates the orifice and the intramural portion of the anomalous RCA and does not manipulate the interarterial course. This case was previously reported elsewhere.19) PA: pulmonary artery, Ao: aorta, MPR: multiplanar reconstruction, RCA: right coronary artery.
Reference
-
1. Yamanaka O, Hobbs RE. Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. Cathet Cardiovasc Diagn. 1990. 21:28–40.2. Kardos A, Babai L, Rudas L, et al. Epidemiology of congenital coronary artery anomalies: a coronary arteriography study on a central European population. Cathet Cardiovasc Diagn. 1997. 42:270–275.3. Topaz O, DeMarchena EJ, Perin E, Sommer LS, Mallon SM, Chahine RA. Anomalous coronary arteries: angiographic findings in 80 patients. Int J Cardiol. 1992. 34:129–138.4. Garg N, Tewari S, Kapoor A, Gupta DK, Sinha N. Primary congenital anomalies of the coronary arteries: a coronary: arteriographic study. Int J Cardiol. 2000. 74:39–46.5. Alexander RW, Griffith GC. Anomalies of the coronary arteries and their clinical significance. Circulation. 1956. 14:800–805.6. Pelliccia A, Spataro A, Maron BJ. Prospective echocardiographic screening for coronary artery anomalies in 1,360 elite competitive athletes. Am J Cardiol. 1993. 72:978–979.7. Pelliccia A. Congenital coronary artery anomalies in young patients: new perspectives for timely identification. J Am Coll Cardiol. 2001. 37:598–600.8. Maron BJ, Thompson PD, Puffer JC, et al. Cardiovascular preparticipation screening of competitive athletes: a statement for health professionals from the Sudden Death Committee (clinical cardiology) and Congenital Cardiac Defects Committee (cardiovascular disease in the young), American Heart Association. Circulation. 1996. 94:850–856.9. Eckart RE, Scoville SL, Campbell CL, et al. Sudden death in young adults: a 25-year review of autopsies in military recruits. Ann Intern Med. 2004. 141:829–834.10. Angelini P. Coronary artery anomalies--current clinical issues: definitions, classification, incidence, clinical relevance, and treatment guidelines. Tex Heart Inst J. 2002. 29:271–278.11. Cheitlin MD, De Castro CM, McAllister HA. Sudden death as a complication of anomalous left coronary origin from the anterior sinus of Valsalva, a not-so-minor congenital anomaly. Circulation. 1974. 50:780–787.12. Liberthson RR, Dinsmore RE, Fallon JT. Aberrant coronary artery origin from the aorta: report of 18 patients, review of literature and delineation of natural history and management. Circulation. 1979. 59:748–754.13. Roberts WC, Siegel RJ, Zipes DP. Origin of the right coronary artery from the left sinus of Valsalva and its functional consequences: analysis of 10 necropsy patients. Am J Cardiol. 1982. 49:863–868.14. Kragel AH, Roberts WC. Anomalous origin of either the right or left main coronary artery from the aorta with subsequent coursing between aorta and pulmonary trunk: analysis of 32 necropsy cases. Am J Cardiol. 1988. 62:771–777.15. Frescura C, Basso C, Thiene G, et al. Anomalous origin of coronary arteries and risk of sudden death: a study based on an autopsy population of congenital heart disease. Hum Pathol. 1998. 29:689–695.16. Taylor AJ, Rogan KM, Virmani R. Sudden cardiac death associated with isolated congenital coronary artery anomalies. J Am Coll Cardiol. 1992. 20:640–647.17. Kaku B, Shimizu M, Yoshio H, et al. Clinical features of prognosis of Japanese patients with anomalous origin of the coronary artery. Jpn Circ J. 1996. 60:731–741.18. Reul RM, Cooley DA, Hallman GL, Reul GJ. Surgical treatment of coronary artery anomalies: report of a 37 1/2-year experience at the Texas Heart Institute. Tex Heart Inst J. 2002. 29:299–307.19. Kim CK, Park CB, Jin U, Lee BY, Song KS. Evaluation of unroofing procedure of anomalous origin of right coronary artery from left sinus of Valsalva between aorta and pulmonary trunk by multidetector computed tomography. J Comput Assist Tomogr. 2005. 29:752–755.20. Kim JY, Yoon SG, Doh JH, et al. Two cases of successful primary percutaneous coronary intervention in patients with an anomalous right coronary artery arising from the left coronary cusp. Korean Circ J. 2008. 38:179–183.21. Moon JY, Jeong CJ, Cho JY, et al. Anomalous origin of a right coronary artery with extrinsic compression between the great vessels: the intravascular ultrasound images. Korean Circ J. 2008. 38:390–392.22. Cha KS, Kim HK, Cun KJ, et al. Role of transesophageal echocardiography in indentifying anomalous origin and course of coronary arteries. Korean Circ J. 1998. 28:576–585.23. Cho HO, Cho KH, Jeong YS, et al. Anomalous origin of the left coronary artery from the right sinus of Valsalva, which presented as acute myocardial infarction. Korean Circ J. 2006. 36:817–819.24. Kim HJ, Kim DK, Won JI, et al. Acute inferior wall myocardial infarction as a result of anomalous origin of the right coronary artery from the left sinus of Valsalva. Korean Circ J. 1997. 27:774–779.25. In : ASCI 2008; –SE36. Abstract.26. Angelini P, Velasco JA, Ott D, Khoshnevis GR. Anomalous coronary artery arising from the opposite sinus: descriptive features and pathophysiologic mechanisms, as documented by intravascular ultrasonography. J Invasive Cardiol. 2003. 15:507–514.27. Taylor AJ, Byers JP, Cheitlin MD, Virmani R. Anomalous right or left coronary artery from the contralateral coronary sinus: "high-risk" abnormalities in the initial coronary artery course and heterogeneous clinical outcomes. Am Heart J. 1997. 133:428–435.28. Virmani R, Chun PK, Goldstein RE, Robinowitz M, McAllister HA. Acute takeoffs of the coronary arteries along the aortic wall and congenital coronary ostial valve-like ridges: association with sudden death. J Am Coll Cardiol. 1984. 3:766–771.29. Angelini P, Velasco JA, Flamm S. Coronary anomalies: incidence, pathophysiology, and clinical relevance. Circulation. 2002. 105:2449–2454.30. Bloomfield P, Erhlich C, Folland ED, Bianco JA, Tow DE, Parisi AF. Anomalous right coronary artery: a surgically correctable cause of angina pectoris. Am J Cardiol. 1983. 51:1235–1237.31. Garcia-Rinaldi R, Sosa J, Olmeda S, Cruz H, Carballido J, Quintana C. Surgical treatment of right coronary arteries with anomalous origin and slit ostium. Ann Thorac Surg. 2004. 77:1525–1529.32. Romp RL, Herlong JR, Landolfo CK, et al. Outcome of unroofing procedure for repair of anomalous aortic origin of left or right coronary artery. Ann Thorac Surg. 2003. 76:589–595.33. Kimbiris D. Anomalous origin of the left main coronary artery from the right sinus of Valsalva. Am J Cardiol. 1985. 55:765–769.34. Jim MH, Siu CW, Ho HH, Miu R, Lee SW. Anomalous origin of the right coronary artery from the left coronary sinus is associated with early development of coronary artery disease. J Invasive Cardiol. 2004. 16:466–468.35. Angelini P, Villason S, Chan AV Jr, Diez JG. Angelini P, editor. Normal and anomalous coronary arteries in humans. Coronary Artery Anomalies: A Comprehensive Approach. 1999. Philadelphia: Lippincott Williams & Wilkins;27–150.36. Zhang F, Ge JB, Qian JY, Fan B, Wang QB, Chen HZ. Frequency of the anomalous coronary origin in the Chinese population with coronary artery stenosis. Zhonghua Nei Ke Za Zhi. 2005. 44:347–349.37. Datta J, White CS, Gilkeson RC, et al. Anomalous coronary arteries in adults: depiction at multi-detector row CT angiography. Radiology. 2005. 235:812–818.38. Kim SY, Seo JB, Do KH, et al. Coronary artery anomalies: classification and ECG-gated multi-detector row CT findings with angiographic correlation. Radiographics. 2006. 26:317–333.39. Shi H, Aschoff AJ, Brambs HJ, Hoffmann MH. Multislice CT imaging of anomalous coronary arteries. Eur Radiol. 2004. 14:2172–2181.40. Schmitt R, Froehner S, Brunn J, et al. Congenital anomalies of the coronary arteries: imaging with contrast-enhanced, multidetector computed tomography. Eur Radiol. 2005. 15:1110–1121.41. van Ooijen PM, Dorgelo J, Zijlstra F, Oudkerk M. Detection, visualization and evaluation of anomalous coronary anatomy on 16-slice multidetector-row CT. Eur Radiol. 2004. 14:2163–2171.42. Lee J, Choe YH, Kim HJ, Park JE. Magnetic resonance imaging demonstration of anomalous origin of the right coronary artery from the left coronary sinus associated with acute myocardial infarction. J Comput Assist Tomogr. 2003. 27:289–291.43. Post JC, van Rossum AC, Bronzwaer JG, et al. Magnetic resonance angiography of anomalous coronary arteries: a new gold standard for delineating the proximal course? Circulation. 1995. 92:3163–3171.44. Bunce NH, Lorenz CH, Keegan J, et al. Coronary artery anomalies: assessment with free-breathing three-dimensional coronary MR angiography. Radiology. 2003. 227:201–208.45. White CS, Laskey WK, Stafford JL, NessAiver M. Coronary MRA: use in assessing anomalies of coronary artery origin. J Comput Assist Tomogr. 1999. 23:203–207.46. Hariharan R, Kacere RD, Angelini P. Can stent-angioplasty be a valid alternative to surgery when revascularization is indicated for anomalous origination of a coronary artery fromthe opposite sinus? Tex Heart Inst J. 2002. 29:308–313.47. Ceyhan C, Tekten T, Onbasili AO. Primary percutaneous coronary intervention of anomalous origin of right coronary artery above the left sinus of Valsalva in a case with acute myocardial infarction: coronary anomalies and myocardial infarction. Int J Cardiovasc Imaging. 2004. 20:293–297.48. Shah AS, Milano CA, Lucke JP. Anomalous origin of the right coronary artery from the left coronary sinus: case report and review of surgical treatments. Cardiovasc Surg. 2000. 8:284–286.49. Gersony WM. Management of anomalous coronary artery from the contralateral coronary sinus. J Am Coll Cardiol. 2007. 50:2083–2084.50. Brothers JA, McBride MG, Seliem MA, et al. Evaluation of myocardial ischemia after surgical repair of anomalous aortic origin of a coronary artery in a series of pediatric patients. J Am Coll Cardiol. 2007. 50:2078–2082.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Sudden Death Associated with Anomalous Left Coronary Artery Origin from Right Sinus of Valsalva with Posterior Course
- Conquering Chaos in ACAOS: Primary Angioplasty in an Anomalous Right Coronary Artery Arising From the Opposite Coronary Sinus
- Congenital Absence of Left Circumflex Coronary Artery: Circumflex Artery Extended from Right Coronary Artery
- Two Cases of Anomalous Origin of Coronary Artery
- Transradial Stenting of an Anomalous Right Coronary Artery Originating from the Left Sinus of Valsalva
