J Korean Acad Prosthodont.
2013 Jul;51(3):160-166. 10.4047/jkap.2013.51.3.160.
Comparative study of fracture strength depending on the occlusal thickness of full zirconia crown
- Affiliations
-
- 1Major in Dentistry, Department of Medical Science, Hanyang University Graduate School, Seoul, Korea. leeys@hanyang.ac.kr
- KMID: 2000164
- DOI: http://doi.org/10.4047/jkap.2013.51.3.160
Abstract
- PURPOSE
The purpose of this study was to compare the fracture strength of traditional metal-ceramic crowns and full zirconia crowns according to the occlusal thickness.
MATERIALS AND METHODS
A mandibular first molar resin tooth was prepared with 1.5 mm occlusal reduction, 1.0 mm rounded shoulder margin and 6degrees taperness in the axial wall. Duplicating the resin tooth, 64 metal dies were fabricated. 48 full zirconia crowns were fabricated using Prettau zirconia blanks by ZIRKONZAHN CAD/CAM and classified into six groups according to the occlusal thickness (0.5 mm, 0.6 mm, 0.7 mm, 0.8 mm, 0.9 mm, 1.0 mm). 16 metal-ceramic crowns were fabricated and classified into two groups according to the occlusal porcelain thickness (1.0 mm, 1.5 mm). All crowns were cemented on each metal die and mounted in a universal testing machine. The load was directed at the functional cusp of each specimen until catastrophic failure occurred. One-way ANOVA, Tukey multiple comparison test (alpha=.05) and t-test (alpha=.05) were used.
RESULTS
The results were as follows. 1. The test 1 group (646.48 N) showed the lowest fracture strength (P<.05), and the value of the test 2.3.4.5 groups (866.40 N, 978.82 N, 1196.82 N, 1222.41 N) increased as thickness increased, but no significant difference were found with the groups (P>.05). The value of test 6 group (1781.24 N) was significantly higher than those of the other groups (P<.05). 2. There were no significant differences of the fracture strength of metal ceramic crowns according to occlusal porcelain thickness 1.0 mm (2515.71 N) and 1.5 mm (3473.31 N) (P<.05).
CONCLUSION
Full zirconia crown needs to be 1.0 mm or over in occlusal thickness for the posterior area to have higher fracture strength than maximum bite force.
Keyword
MeSH Terms
Figure
-
Fig. 1. Fabrication process of metal die.

Fig. 2. Full zirconia crown.

Fig. 3. Metal ceramic crown - occlusal porcelain thickness 1.0 mm (left), 1.5 mm (right).
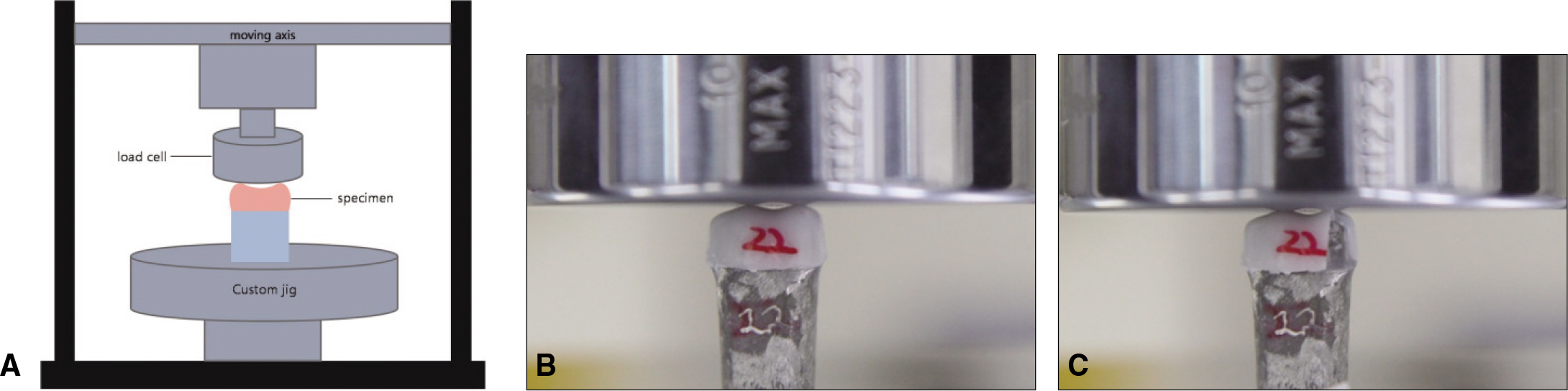
Fig. 4. A: Schematic illustration of the universal test machine experimental setup, B: Secured crown for testing in custom jig on universal testing machine, C: Fractured specimen after loading.
Reference
-
1.Ernsmere JB. Porcelain dental work. Br J Dent Sci. 1900. 43:547–50.2.Weinstein M., Katz S., Weinstein AB. Fused porcelain-to-metal teeth. 1962. US patent 3052, 982.3.Johnston JF. Porcelain veneers bonded to gold castings-A progress report. J Prosthet Dent. 1958. 8:120–2.
Article4.Piddock V., Qualtrough AJ. Dental ceramics-an update. J Dent. 1990. 18:227–35.
Article5.Adair PJ., Grossman DG. The castable ceramic crown. Int J Periodontics Restorative Dent. 1984. 4:32–46.6.Optec HSP laboratory technique manual. Jeneric/Pentro Inc;Wallingford, Conn: 1988.7.Sadoun M. All ceramic bridges with the slip casting technique. Presented at the 7tb International Symposium on Ceramics. Paris, September,. 1988.8.Beham G. IPS-Empress: a new ceramic technology. ZWR. 1991. 100:404–8.9.Garvie RC., Hannik RH., Pascoe RT. Ceramic Steel? Nature. 1975. 258:703–4.
Article10.Filser F., Kocher P., Gauckler LJ. Net-shaping of ceramic components by direct ceramic machining. Assembly Autom. 2003. 23:382–90.
Article11.Heintze SD., Rousson V. Survival of zirconia- and metal-supported fixed dental prostheses: a systematic review. Int J Prosthodont. 2010. 23:493–502.12.Bachhav VC., Aras MA. Zirconia-based fixed partial dentures: a clinical review. Quintessence Int. 2011. 42:173–82.13.Ozkurt Z., Kazazoğlu E. Clinical success of zirconia in dental applications. J Prosthodont. 2010. 19:64–8.14.Sailer I., Fehe′r A., Filser F., Lu¨thy H., Gauckler LJ., Scha¨rer P., Franz Ha¨mmerle CH. Prospective clinical study of zirconia posterior fixed partial dentures: 3-year follow-up. Quintessence Int. 2006. 37:685–93.15.Molin MK., Karlsson SL. Five-year clinical prospective evaluation of zirconia-based Denzir 3-unit FPDs. Int J Prosthodont. 2008. 21:223–7.16.Craig RG., Powers JM. Restorative dental materials. 8th ed.St Louis, Mo: The CV Mosby Co;1989.17.Waltimo A., Ko¨no¨nen M. Maximal bite force and its association with signs and symptoms of craniomandibular disorders in young Finnish non-patients. Acta Odontol Scand. 1995. 53:254–8.
Article18.Waltimo A., Nystro¨m M., Ko¨no¨nen M. Bite force and dentofacial morphology in men with severe dental attrition. Scand J Dent Res. 1994. 102:92–6.
Article19.Ferrario VF., Sforza C., Zanotti G., Tartaglia GM. Maximal bite forces in healthy young adults as predicted by surface electromyography. J Dent. 2004. 32:451–7.
Article20.Brukl CE., Ocampo RR. Compressive strengths of a new foil and porcelain-fused-to-metal crowns. J Prosthet Dent. 1987. 57:404–10.
Article21.Lee SM., Jeong HC., Jeon YC. Fracture strength of zirconia monolithic crowns and metal-ceramic crowns after cyclic loading and thermocycling. J Korean Acad Prosthodont. 2007. 45:12–20.22.Shin MR., Kim MJ., Oh SC. Fracture load and marginal fitness of zirconia ceramic coping by design and coloration. J Korean Acad Prosthodont. 2009. 47:406–15.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Fracture strength of zirconia monolithic crowns
- Fracture Strength and Translucency of CAD/CAM Zirconia Crown for Primary Anterior Tooth
- The effect of reduced thickness in different regions on the fracture resistance of monolithic zirconia crowns
- Fracture strength of zirconia monolithic crowns and metal-ceramic crowns after cyclic loading and thermocycling
- A comparative study on the fracture behavior of zironia, glass infiltrated alumina and PFM full crown system
