Obstet Gynecol Sci.
2015 Jan;58(1):10-16. 10.5468/ogs.2015.58.1.10.
Midtrimester maternal plasma concentrations of angiopoietin 1, angiopoietin 2, and placental growth factor in pregnant women who subsequently develop preeclampsia
- Affiliations
-
- 1Department of Obstetrics and Gynecology, Jeju National University School of Medicine, Jeju, Korea.
- 2Department of Obstetrics and Gynecology, Seoul National University College of Medicine, Seoul, Korea. jhs0927@snu.ac.kr
- KMID: 1994221
- DOI: http://doi.org/10.5468/ogs.2015.58.1.10
Abstract
OBJECTIVE
The aim of this study was to compare midtrimester maternal plasma concentrations of angiopoietin 1, angiopoietin 2, and placental growth factor between pregnant women who subsequently developed preeclampsia and those who did not.
METHODS
Midtrimester maternal plasma was collected and stored at -70degrees C when genetic amniocentesis was performed. Cases included 37 samples of individual who subsequently developed preeclampsia, and matched controls were from individuals who did not develop preeclampsia. Angiopoietin 1, angiopoietin 2, and placental growth factor concentrations were measured by the enzyme-linked immunosorbent assay method and were compared using the Mann-Whitney U-test. A P-value <0.05 was considered significant.
RESULTS
In pregnant women who subsequently developed preeclampsia, midtrimester maternal plasma concentrations of angiopoietin 1 and angiopoietin 2 were significantly higher and placental growth factor concentrations were significantly lower than in women who did not develop preeclampsia (angiopoietin 1: 10.6 [3.1-19.7] vs. 7.8 [0.9-24.4] ng/mL, P=0.031; angiopoietin 2: 31.0 [4.7-81.2] vs. 18.4 [4.2-49.7] ng/mL, P<0.001; placental growth factor: 87.1 [14.2-774.3] vs. 148.8 [57.2-425.6] pg/mL, P<0.001). Within the case group who subsequently developed preeclampsia, the placental growth factor was significantly lower in those who had fetal growth restrictions than in those who did not (placental growth factor: 72.5 [14.2-774.3] vs. 140.9 [44.2-257.5] pg/mL, P=0.003).
CONCLUSION
Midtrimester maternal plasma concentrations of angiopoietin 1, angiopoietin 2, and placental growth factor may be associated with the subsequent development of preeclampsia.
MeSH Terms
Figure
-
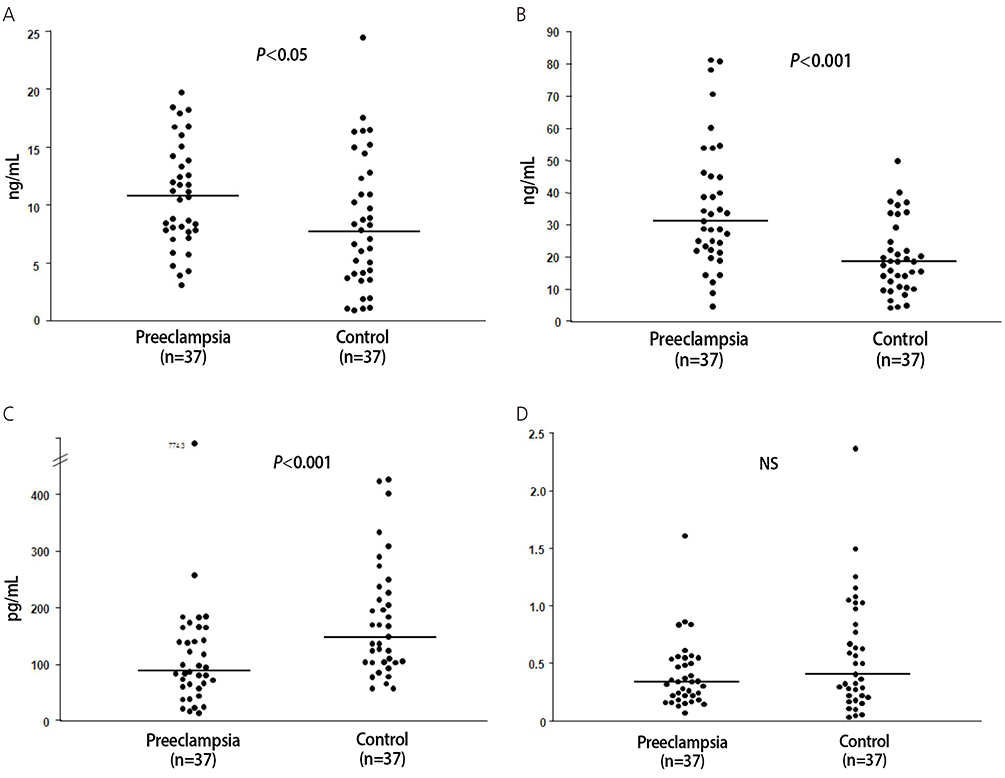
Fig. 1 Midtrimester maternal plasma concentrations of angiopoietin 1 (A), angiopoietin 2 (B), placental growth factor (C), and angiopoietin 1/angiopoietin 2 ratio (D) in patients who subsequently developed preeclampsia and controls. In pregnant women who subsequently developed preeclampsia, midtrimester maternal plasma concentrations of angiopoietin 1 and angiopoietin 2 were significantly higher and placental growth factor concentrations were significantly lower than those who did not develop preeclampsia. NS, non-significant.
Cited by 1 articles
-
Maternal Plasma Angiopoietin-1 and Angiopoietin-2 in Pregnant Women with Chronic Hypertension
Eunjin Kim, Minji Kang, Jong Kwan Jun
Korean J Perinatol. 2015;26(1):28-34. doi: 10.14734/kjp.2015.26.1.28.
Reference
-
1. ACOG Committee on Obstetric Practice. ACOG practice bulletin. Diagnosis and management of preeclampsia and eclampsia. Number 33, January 2002. American College of Obstetricians and Gynecologists. Int J Gynaecol Obstet. 2002; 77:67–75.2. Sibai B, Dekker G, Kupferminc M. Pre-eclampsia. Lancet. 2005; 365:785–799.3. Erez O, Romero R, Espinoza J, Fu W, Todem D, Kusanovic JP, et al. The change in concentrations of angiogenic and antiangiogenic factors in maternal plasma between the first and second trimesters in risk assessment for the subsequent development of preeclampsia and small-for-gestational age. J Matern Fetal Neonatal Med. 2008; 21:279–287.4. Maynard SE, Min JY, Merchan J, Lim KH, Li J, Mondal S, et al. Excess placental soluble fms-like tyrosine kinase 1 (sFlt1) may contribute to endothelial dysfunction, hypertension, and proteinuria in preeclampsia. J Clin Invest. 2003; 111:649–658.5. Levine RJ, Maynard SE, Qian C, Lim KH, England LJ, Yu KF, et al. Circulating angiogenic factors and the risk of preeclampsia. N Engl J Med. 2004; 350:672–683.6. Park CW, Park JS, Shim SS, Jun JK, Yoon BH, Romero R. An elevated maternal plasma, but not amniotic fluid, soluble fms-like tyrosine kinase-1 (sFlt-1) at the time of mid-trimester genetic amniocentesis is a risk factor for preeclampsia. Am J Obstet Gynecol. 2005; 193(3 Pt 2):984–989.7. Karamysheva AF. Mechanisms of angiogenesis. Biochemistry (Mosc). 2008; 73:751–762.8. Romero R, Nien JK, Espinoza J, Todem D, Fu W, Chung H, et al. A longitudinal study of angiogenic (placental growth factor) and anti-angiogenic (soluble endoglin and soluble vascular endothelial growth factor receptor-1) factors in normal pregnancy and patients destined to develop preeclampsia and deliver a small for gestational age neonate. J Matern Fetal Neonatal Med. 2008; 21:9–23.9. Nadar SK, Karalis I, Al Yemeni E, Blann AD, Lip GY. Plasma markers of angiogenesis in pregnancy induced hypertension. Thromb Haemost. 2005; 94:1071–1076.10. Leinonen E, Wathen KA, Alfthan H, Ylikorkala O, Andersson S, Stenman UH, et al. Maternal serum angiopoietin-1 and -2 and tie-2 in early pregnancy ending in preeclampsia or intrauterine growth retardation. J Clin Endocrinol Metab. 2010; 95:126–133.11. Geva E, Ginzinger DG, Zaloudek CJ, Moore DH, Byrne A, Jaffe RB. Human placental vascular development: vasculogenic and angiogenic (branching and nonbranching) transformation is regulated by vascular endothelial growth factor-A, angiopoietin-1, and angiopoietin-2. J Clin Endocrinol Metab. 2002; 87:4213–4224.12. Zhang EG, Smith SK, Baker PN, Charnock-Jones DS. The regulation and localization of angiopoietin-1, -2, and their receptor Tie2 in normal and pathologic human placentae. Mol Med. 2001; 7:624–635.13. Hirokoshi K, Maeshima Y, Kobayashi K, Matsuura E, Sugiyama H, Yamasaki Y, et al. Increase of serum angiopoietin-2 during pregnancy is suppressed in women with preeclampsia. Am J Hypertens. 2005; 18(9 Pt 1):1181–1188.14. Hirokoshi K, Maeshima Y, Kobayashi K, Matsuura E, Sugiyama H, Yamasaki Y, et al. Elevated serum sFlt-1/Ang-2 ratio in women with preeclampsia. Nephron Clin Pract. 2007; 106:c43–c50.15. Bolin M, Wiberg-Itzel E, Wikstrom AK, Goop M, Larsson A, Olovsson M, et al. Angiopoietin-1/angiopoietin-2 ratio for prediction of preeclampsia. Am J Hypertens. 2009; 22:891–895.16. Wang Y, Tasevski V, Wallace EM, Gallery ED, Morris JM. Reduced maternal serum concentrations of angiopoietin-2 in the first trimester precede intrauterine growth restriction associated with placental insufficiency. BJOG. 2007; 114:1427–1431.17. Schneuer FJ, Roberts CL, Ashton AW, Guilbert C, Tasevski V, Morris JM, et al. Angiopoietin 1 and 2 serum concentrations in first trimester of pregnancy as biomarkers of adverse pregnancy outcomes. Am J Obstet Gynecol. 2014; 210:345.e1–345.e9.18. Maisonpierre PC, Suri C, Jones PF, Bartunkova S, Wiegand SJ, Radziejewski C, et al. Angiopoietin-2, a natural antagonist for Tie2 that disrupts in vivo angiogenesis. Science. 1997; 277:55–60.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Maternal Plasma Angiopoietin-1 and Angiopoietin-2 in Pregnant Women with Chronic Hypertension
- Maternal Plasma Hepatocyte Growth Factor Concentrations in Women Who Subsequently Developed Preeclampsia
- Analysis of HLA-G expression in preeclampsia and intrauterine growth restriction
- Hypertension, Vascular Rarefaction and Angiopoietin-1
- Pathogenesis and promising non-invasive markers for preeclampsia
