Small (<4 cm), Unclassified Renal Cell Carcinoma Presenting with Initial Bone Metastasis: A Case of a Metastatic Lesion Missed at the Initial Diagnosis
- Affiliations
-
- 1Department of Urology, Chonnam National University Medical School, Gwangju, Korea. urohwang@gmail.com
- 2Department of Hematology-Oncology, Chonnam National University Medical School, Gwangju, Korea.
- 3Department of Pathology, Chonnam National University Medical School, Gwangju, Korea.
- KMID: 1988737
- DOI: http://doi.org/10.4111/kju.2012.53.12.883
Abstract
- A 49-year-old man presented with an incidentally detected right renal mass on a health examination. The abdominal computed tomography and magnetic resonance imaging showed a 3-cm right renal mass suspected of being a hypovascular tumor, such as papillary renal cell carcinoma, and an osteoblastic metastatic lesion on the right iliac bone. However, we missed a bone lesion at the time of diagnosis. A laparoscopic radical nephrectomy was performed and the final pathology confirmed unclassified renal cell carcinoma. The follow-up imaging studies showed several neck lymph nodes and multiple bone metastases at the lumbar spine, right iliac bone, and left femur. Thirteen cycles of temsirolimus were administered to the patient, but follow-up positron emission tomography showed newly developed liver and left adrenal metastasis and increased bone metastasis. It is important to note that T1a renal cell carcinoma can present with distant metastasis and thus demands scrupulous examination even though the tumor size may be small.
MeSH Terms
Figure
-

FIG. 1 Pretreatment computed tomography scan showing a 3-cm tumor of the right kidney and an osteoblastic lesion on the right iliac bone (arrow).

FIG. 2 Gross and microscopic findings. (A) The mass was located within the cortex of the kidney and was 3.0×2.0×2.0 cm in size. There was no evidence of cystic change, hemorrhage, or necrosis in the mass. (B) The tumor cells were arranged in solid sheets. The cells were polygonal and the nuclei were moderately hyperchromatic. There was no evidence of clear cells, papillary, or acinar structures (H&E, ×200). (C) Most of the tumor cells were negative for CD10 (×200). (D) The tumor cells displayed diffuse positivity for vimentin (×200).
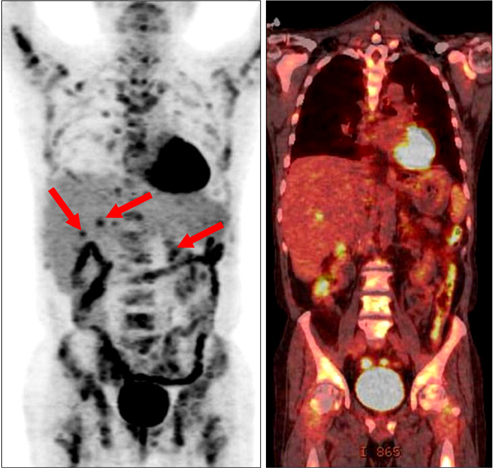
FIG. 3 The latest follow-up positron emission tomography. Newly developed liver and left adrenal metastases (arrow, focal hypermetabolism) and increased bone metastasis were evident.
Reference
-
1. Chow WH, Devesa SS, Warren JL, Fraumeni JF Jr. Rising incidence of renal cell cancer in the United States. JAMA. 1999. 281:1628–1631.2. Klatte T, Patard JJ, de Martino M, Bensalah K, Verhoest G, de la Taille A, et al. Tumor size does not predict risk of metastatic disease or prognosis of small renal cell carcinomas. J Urol. 2008. 179:1719–1726.3. Karakiewicz PI, Hutterer GC, Trinh QD, Pantuck AJ, Klatte T, Lam JS, et al. Unclassified renal cell carcinoma: an analysis of 85 cases. BJU Int. 2007. 100:802–808.4. Pantuck AJ, Zisman A, Belldegrun AS. The changing natural history of renal cell carcinoma. J Urol. 2001. 166:1611–1623.5. Ljungberg B, Cowan NC, Hanbury DC, Hora M, Kuczyk MA, Merseburger AS, et al. EAU guidelines on renal cell carcinoma: the 2010 update. Eur Urol. 2010. 58:398–406.6. Lopez-Beltran A, Scarpelli M, Montironi R, Kirkali Z. 2004 WHO classification of the renal tumors of the adults. Eur Urol. 2006. 49:798–805.7. Zisman A, Chao DH, Pantuck AJ, Kim HJ, Wieder JA, Figlin RA, et al. Unclassified renal cell carcinoma: clinical features and prognostic impact of a new histological subtype. J Urol. 2002. 168:950–955.8. Crispen PL, Tabidian MR, Allmer C, Lohse CM, Breau RH, Blute ML, et al. Unclassified renal cell carcinoma: impact on survival following nephrectomy. Urology. 2010. 76:580–586.9. Hudes G, Carducci M, Tomczak P, Dutcher J, Figlin R, Kapoor A, et al. Temsirolimus, interferon alfa, or both for advanced renal-cell carcinoma. N Engl J Med. 2007. 356:2271–2281.10. Rodriguez Faba O, Breda A, Rosales A, Palou J, Algaba F, Maroto Rey P, et al. Neoadjuvant temsirolimus effectiveness in downstaging advanced non-clear cell renal cell carcinoma. Eur Urol. 2010. 58:307–310.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Metastatic Renal Cell Carcinoma to the Gallbladder
- (99m)Tc-HDP Bone Scintigraphy Finding of Metastatic Renal Cell Carcinoma Bone Lesion Changed from Hot to Cold Lesion: Comparing with (18)F-FDG PET/CT
- Cytologic Diagnosis of Metastatic Hepatocellular Carcinoma by Aspiration Cytology of Sacrum
- Can Initial 18F-FDG PET-CT Imaging Give Information onMetastasis in Patients with Primary Renal Cell Carcinoma?
- A Case of Subcutaneous Tissue Metastasis of Renal Cell Carcinoma
