Korean J Urol.
2014 May;55(5):363-366. 10.4111/kju.2014.55.5.363.
Large Bilateral Adrenal Leiomyomas Presenting as Calcified Adrenal Masses: A Rare Case Report
- Affiliations
-
- 1Department of Urology, Post Graduate Institute of Medical Education and Research, Chandigarh, India. santoshsp1967jaimatadi@yahoo.co.in
- 2Department of Histopathology, Post Graduate Institute of Medical Education and Research, Chandigarh, India.
- KMID: 1988416
- DOI: http://doi.org/10.4111/kju.2014.55.5.363
Abstract
- We report the case of a 55-year-old woman with bilateral, large, calcified adrenal tumors who was treated by laparoscopic adrenalectomy. The patient presented with upper abdominal discomfort for the past 5 years. Her imaging showed bilateral enlarged adrenal glands up to 10-cm size with punctate calcifications. Positron emission tomography scan demonstrated moderate fluorodeoxyglucose avidity in the left adrenal mass. Bilateral laparoscopic adrenalectomy was performed through a transperitoneal approach. The postoperative period was uneventful, and the patient was discharged on the third postoperative day. Histology findings were consistent with adrenal leiomyomatosis.
Keyword
MeSH Terms
Figure
-

FIG. 1 Contrast-enhanced computed tomography of the abdomen showing bilateral calcified adrenal masses.
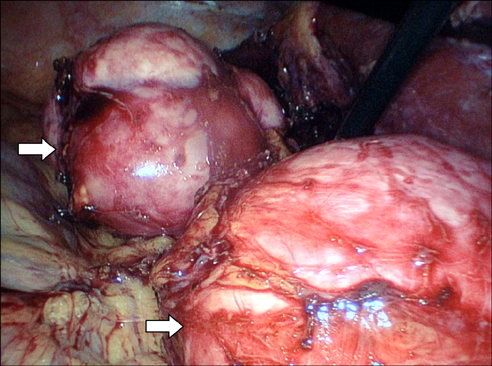
FIG. 2 Intraoperative photographs showing the left adrenal tumor being dissected. Arrows indicating adrenal tumor.

FIG. 3 Gross pathology specimen showing bilateral firm, lobulated, well-encapsulated adrenal tumor.

FIG. 4 (A) Normal adrenal gland seen at the periphery with encapsulated tumor arranged in long and short fascicles (H&E, ×40). (B) Higher magnification showing fascicles of benign spindle-shaped cells with minimal nuclear atypia (H&E, ×200). (C) Neoplastic cells showing strong positivity with smooth muscle actin (immunoperoxidase, ×200).
Reference
-
1. Brunt LM, Moley JF. Adrenal incidentaloma. World J Surg. 2001; 25:905–913.2. Hindman N, Israel GM. Adrenal gland and adrenal mass calcification. Eur Radiol. 2005; 15:1163–1167.3. Jacobs IA, Kagan SA. Adrenal leiomyoma: a case report and review of the literature. J Surg Oncol. 1998; 69:111–112.4. Parola P, Petit N, Azzedine A, Dhiver C, Gastaut JA. Symptomatic leiomyoma of the adrenal gland in a woman with AIDS. AIDS. 1996; 10:340–341.5. Jimenez-Heffernan JA, Hardisson D, Palacios J, Garcia-Viera M, Gamallo C, Nistal M. Adrenal gland leiomyoma in a child with acquired immunodeficiency syndrome. Pediatr Pathol Lab Med. 1995; 15:923–929.6. Jacobs JK, Goldstein RE, Geer RJ. Laparoscopic adrenalectomy: a new standard of care. Ann Surg. 1997; 225:495–501.7. Gagner M, Lacroix A, Bolte E, Pomp A. Laparoscopic adrenalectomy. The importance of a flank approach in the lateral decubitus position. Surg Endosc. 1994; 8:135–138.8. Nguyen PH, Keller JE, Novitsky YW, Heniford BT, Kercher KW. Laparoscopic approach to adrenalectomy: review of perioperative outcomes in a single center. Am Surg. 2011; 77:592–596.
