Atrial Septal Defect with Normal Pulmonary Arterial Pressure in Adult Cyanotic Patient
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Keimyung University Dongsan Medical Center, Daegu, Korea. khyungseop@dsmc.or.kr
- 2Department of Thoracic Surgery, Keimyung University Dongsan Medical Center, Daegu, Korea.
- KMID: 1980427
- DOI: http://doi.org/10.4250/jcu.2014.22.4.220
Abstract
- A 22-year-old male presented with recurrent stroke, central cyanosis, and dyspnea. Transesophageal echocardiography and cardiac catheterization revealed bidirectional shunt flow through atrial septal defect (ASD) without pulmonary arterial hypertension. The orifice of inferior vena cava facing towards ASD opening led partially right to left shunt resulting in cyanosis with normal pulmonary arterial pressure.
Keyword
MeSH Terms
Figure
-
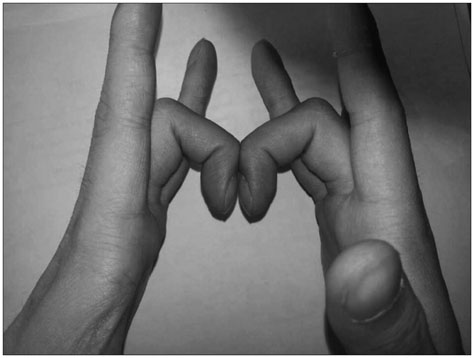
Fig. 1 Clubbing finger of the patient (absence of normal diamond shaped Schamroth's window between two opposite nailbeds, which indicates positive Schamroth's test).
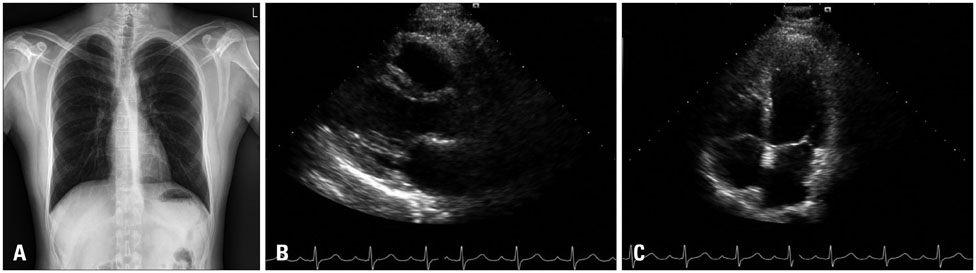
Fig. 2 Initial chest X-ray (A) and transthoracic echocardiography of parasternal long axis (B) and apical 4-chamber view (C). These tests showed that cardiac chambers were not enlarged and left ventricular ejection fraction was normal.
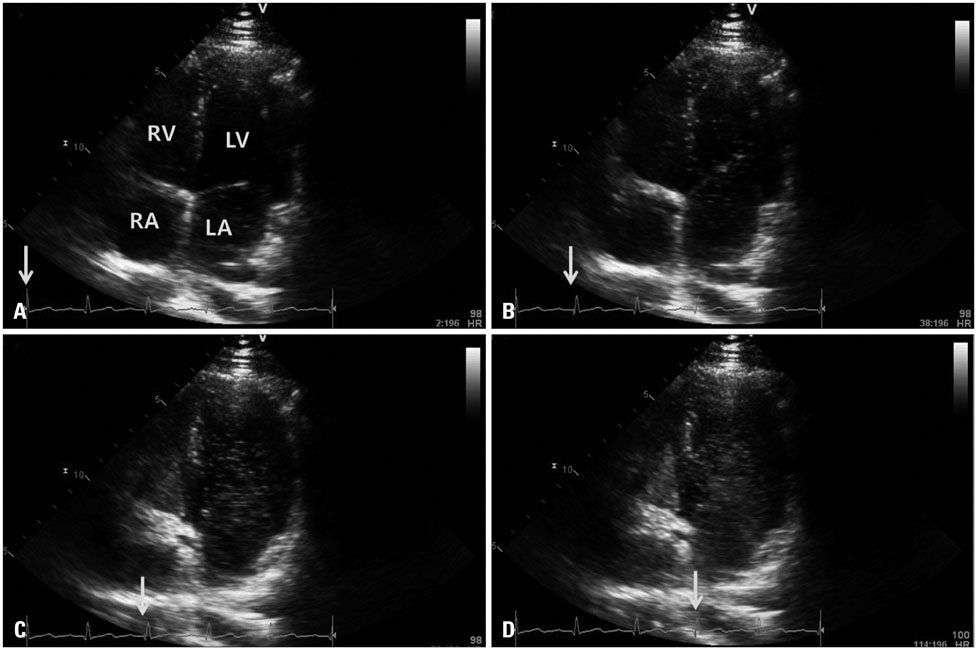
Fig. 3 Transthoracic echocardiography with agitated saline bubble test in modified apical 4-chamber view. Filling of LV cavity with bubble starts at the same time when RV cavity is filled (A and B), LV fulfillment is finished within 4 beats immediately after appearance of RV bubble (C and D). Arrow indicates each cardiac cycle of the image. RV: right ventricle, LV: left ventricle, RA: right atrium, LA: left atrium.
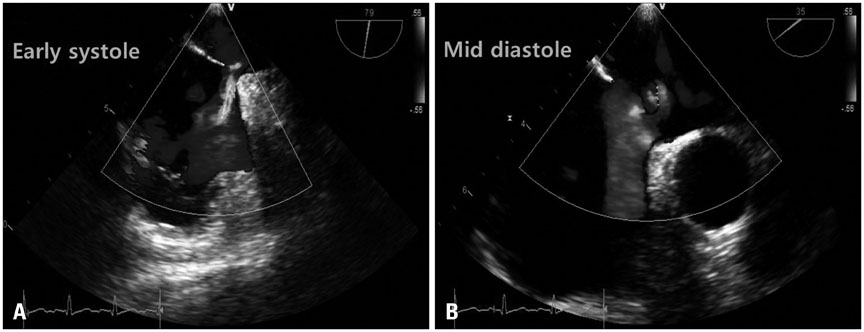
Fig. 4 Transesophageal echocardiography with color Doppler imaging during early systole (A) and mid-diastole (B).
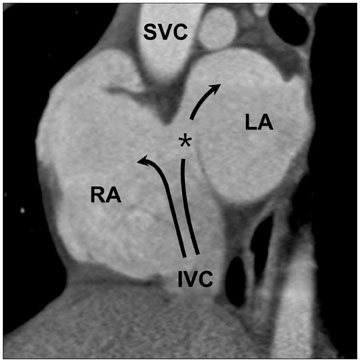
Fig. 5 Sagittal view of heart dynamic computed tomography reveals that inferior vena cava flow (arrow) drains partially towards left atrium via atrial septal defect (asterisk). IVC: inferior vena cava, LA: left atrium, RA: right atrium, SVC: superior vena cava.
Reference
-
1. Sommer RJ, Hijazi ZM, Rhodes JF Jr. Pathophysiology of congenital heart disease in the adult: part I: Shunt lesions. Circulation. 2008; 117:1090–1099.
Article2. Godart F, Rey C, Prat A, Vincentelli A, Chmaït A, Francart C, Porte H. Atrial right-to-left shunting causing severe hypoxaemia despite normal right-sided pressures. Report of 11 consecutive cases corrected by percutaneous closure. Eur Heart J. 2000; 21:483–489.
Article3. Frost AE, Quiñones MA, Zoghbi WA, Noon GP. Reversal of pulmonary hypertension and subsequent repair of atrial septal defect after treatment with continuous intravenous epoprostenol. J Heart Lung Transplant. 2005; 24:501–503.
Article4. Steele PM, Fuster V, Cohen M, Ritter DG, McGoon DC. Isolated atrial septal defect with pulmonary vascular obstructive disease--long-term follow-up and prediction of outcome after surgical correction. Circulation. 1987; 76:1037–1042.
Article5. Thomas JD, Tabakin BS, Ittleman FP. Atrial septal defect with right to left shunt despite normal pulmonary artery pressure. J Am Coll Cardiol. 1987; 9:221–224.
Article6. Nazzal SB, Bansal RC, Fitzmorris SJ, Schmidt CA. Platypnea-orthodeoxia as a cause of unexplained hypoxemia in an 82-yr-old female. Cathet Cardiovasc Diagn. 1990; 19:242–245.
Article7. Bakris NC, Siddiqi AJ, Fraser CD Jr, Mehta AC. Right-to-left interatrial shunt after pneumonectomy. Ann Thorac Surg. 1997; 63:198–201.
Article8. Smeenk FW, Postmus PE. Interatrial right-to-left shunting developing after pulmonary resection in the absence of elevated right-sided heart pressures. Review of the literature. Chest. 1993; 103:528–531.
Article9. Kizer JR, Devereux RB. Clinical practice. Patent foramen ovale in young adults with unexplained stroke. N Engl J Med. 2005; 353:2361–2372.
Article10. Frizzell JP. Acute stroke: pathophysiology, diagnosis, and treatment. AACN Clin Issues. 2005; 16:421–440. quiz 597-8.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The effect of perioperative inhaled iloprost on congenital heart disease with severe pulmonary arterial hypertension
- Pulmonary arterial hypertension in congenital heart disease: correlation of radiologic index with hemodynamicdata
- A Case of Atrial Septal Defect in Identical Twins
- Surgical treatment of atrial septal defect in adult patients
- Pulmonary Arterial Thrombosis in a Patient With an Atrial Septal Defect and Eisenmenger Syndrome
