Pulmonary Artery Stenosis due to Lung Carcinoma: A Rare Cause of Dyspnea
- Affiliations
-
- 1Department of Cardiology, King George's Medical University, Lucknow, Uttar Pradesh, India. raj_iv_infusion@yahoo.co.in
- KMID: 1980425
- DOI: http://doi.org/10.4250/jcu.2014.22.4.209
Abstract
- Acquired bilateral pulmonary artery stenosis in adults due to lung malignancy is infrequently reported. We describe an adult male who presented to us with chief complaints of dyspnea on exertion and one episode of hemoptysis. Two dimensional transthoracic echocardiography with color Doppler showed presence of an extra cardiac mass causing severe extrinsic compression of both the right and left pulmonary artery leading to high pressure severe tricuspid regurgitation and extension of the mass into the left atrium. Three dimensional transthoracic echocardiography clearly delineated the anatomy of the left atrial mass and its surrounding anatomical relationship. The diagnosis of non small cell lung carcinoma was confirmed by multidetector computed tomography (MDCT) and with MDCT guided biopsy with histopathology. Patient succumbed one month later due to an episode of massive hemoptysis.
MeSH Terms
Figure
-

Fig. 1 Chest X-ray PA view showing an opaque shadow in the upper and middle zone of the left lung which is inseparable from the cardiac silhoute. Also note that the left hemi-diaphragm is higher than the right hemi-diaphragm.
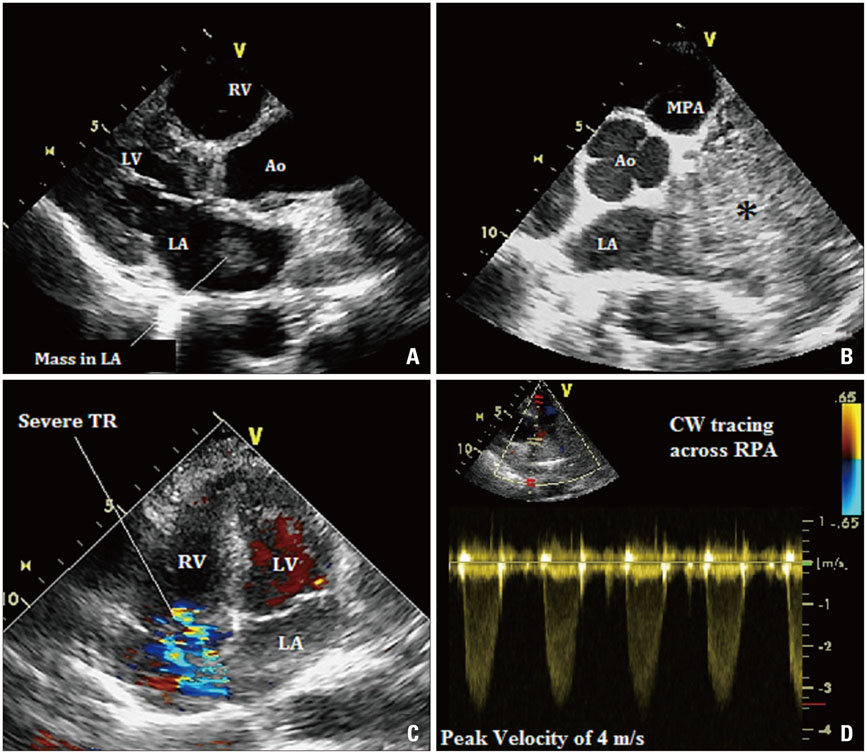
Fig. 2 Two dimensional transthoracic echocardiography with color Doppler. The parasternal long axis view (A) is showing a mass in the left atrium. The extracardiac mass (indicated by *) is seen to involve the region of the MPA and right and the left pulmonary artery region in the basal short axis view (B). Severe tricuspid regurgitation is seen in the apical four chamber view (C) with a peak TR velocity of 4.2 m/sec on continous wave Doppler (D). Ao: aorta, LA: left atrium, LV: left ventricle, MPA: main pulmonary artery, RV: right ventricle, TR: tricuspid regurgitation, RPA: right pulmonary artery.
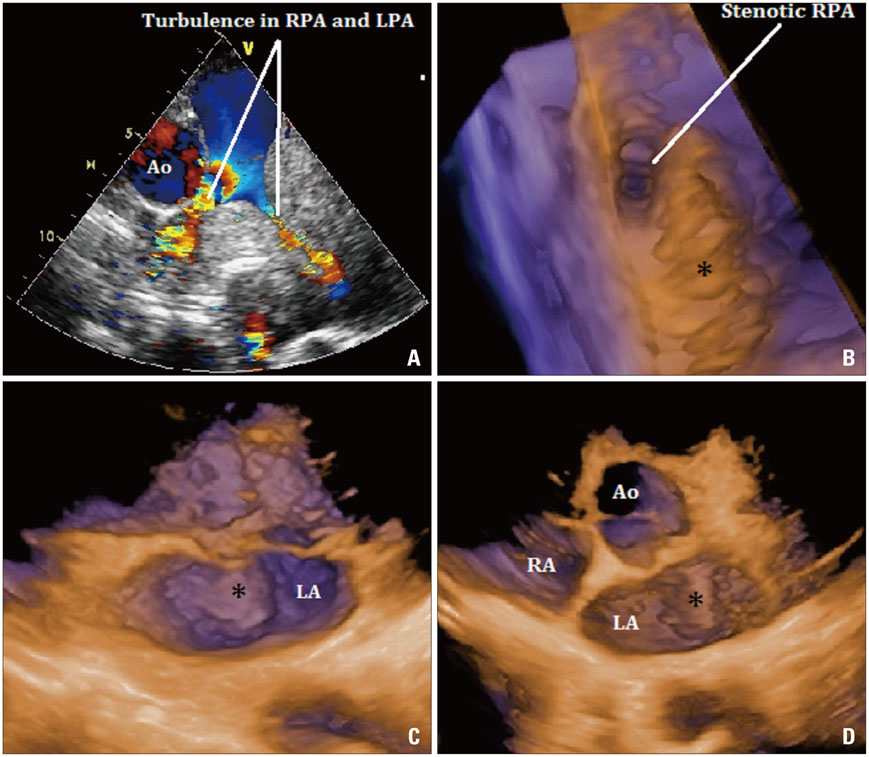
Fig. 3 Two dimensional transthoracic echocardiography with color Doppler. The basal short axis (A) view with focus on the pulmonary artery showing severe turbulence in RPA and LPA caused by extrinsic compression of a huge mass. Three dimensional transthoracic echocardiography showing stenotic right pulmonary artery caused by the extrinsic compression by the mass (B) and the surface characteristics and anatomical relationship of the intra atrial extension of the mass (indicated by * in C and D). Ao: aorta, LA: left atrium, LPA: left pulmonary artery, RA: right atrium, RPA: right pulmonary artery.

Fig. 4 Multidetector computed tomography with contrast showing a large mass (indicated by *) in the upper left pulmonary zone encroaching upon and causing severe extrinsic compression of the RPA and LPA as shown in the axial sections (A and B). The mass has infiltrated into the left atrium in the form of a pedunculated growth as seen in the axial section (C) and in the coronal section (D). AA: ascending aorta, DA: descending aorta, LA: left atrium, LPA: left pulmonary artery, RPA: right pulmonary artery, MPA: main pulmonary artery.
Reference
-
1. Viseur P, Unger P. Doppler echocardiographic diagnosis and follow-up of acquired pulmonary stenosis due to external cardiac compression. Cardiology. 1995; 86:80–82.
Article2. American College of Cardiology. American Heart Association Task Force on Practice Guidelines (Writing Committee to revise the 1998 guidelines for the management of patients with valvular heart disease). Society of Cardiovascular Anesthesiologists. Bonow RO, Carabello BA, Chatterjee K, de Leon AC Jr, Faxon DP, Freed MD, Gaasch WH, Lytle BW, Nishimura RA, O'Gara PT, O'Rourke RA, Otto CM, Shah PM, Shanewise JS, Smith SC Jr, Jacobs AK, Adams CD, Anderson JL, Antman EM, Fuster V, Halperin JL, Hiratzka LF, Hunt SA, Lytle BW, Nishimura R, Page RL, Riegel B. 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (writing Committee to Revise the 1998 guidelines for the management of patients with valvular heart disease) developed in collaboration with the Society of Cardiovascular Anesthesiologists endorsed by the Society for Cardiovascular Angiography and Interventions and the Society of Thoracic Surgeons. J Am Coll Cardiol. 2006; 48:e1–e148.3. Plana JC. Three-dimensional echocardiography to assess intra-cardiac masses. In : Badano LP, Lang RM, Zamorano JL, editors. Textbook of real-time three dimensional echocardiography. London: Springer-Verlag;2011. p. 111–119.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Air Way Instability due to Pulmonary Artery Sling combined with Diffuse Tracheal Stenosis
- Acquired pulmonary stenosis secondary to tuberculosis: A Case Report
- Stenosis of Individual Pulmonary Veins
- Pulmonary Artery Sling with Situs Solitus Dextroposition of Heart and Left Superior Vena Cava
- Unilateral Absence of Pulmonary Artery
