Prognostic Implications of Right and Left Atrial Enlargement after Radiofrequency Catheter Ablation in Patients with Nonvalvular Atrial Fibrillation
- Affiliations
-
- 1Cardiology Division, Department of Internal Medicine, Gachon University of Medicine and Science, Incheon, Korea.
- 2Department of Radiology, Research Institute of Radiological Science, Yonsei University College of Medicine, Seoul, Korea.
- 3Division of Cardiology, Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea. cby6908@yuhs.ac
- KMID: 1964102
- DOI: http://doi.org/10.4070/kcj.2015.45.4.301
Abstract
- BACKGROUND AND OBJECTIVES
The prognostic role of the right atrium (RA) compared with that of the left atrium (LA) is unclear in patients with atrial fibrillation (AF). We assessed structural changes in both atria and determined their association with recurrence of AF after radiofrequency catheter ablation (RFCA).
SUBJECTS AND METHODS
All 111 patients with nonvalvular AF (87 men; mean age, 57+/-11 years; 68 with paroxysmal AF) who underwent RFCA were enrolled consecutively. Three-dimensional volumes of both atria measured from computed tomography images were compared between subjects with and without recurrence of AF during the follow-up.
RESULTS
Early (<3 months), 6-month, and 1-year recurrence was documented in 26 (24%), 30 (27%), and 36 (32%) patients, respectively. Significantly larger RA and LA volume indices (RAVI and LAVI) were observed in the early, 6-month, and 1-year recurrence groups (p<0.05 for all). In multivariate analysis, Early recurrence was independently associated with RAVI (for each 10 mL/m2 increase; odds ratio [OR], 1.31; 95% confidence interval [CI], 1.03-1.66, p= 0.03), but not with LAVI. However, both RAVI and LAVI failed to predict 6-month outcomes independently. LAVI was the only independent predictor of 1-year recurrence (for each 10 mL/m2 increase; OR, 1.36; 95% CI, 1.08-1.71, p=0.009).
CONCLUSION
RA enlargement was more closely related to early recurrence of AF after RFCA than LA size. However, LA size, rather than RA volume, was a determinant of long-term AF prognosis after RFCA. These findings suggest a temporal pattern in the prognostic implication of enlargement in each atrium that switches over time after RFCA for AF.
MeSH Terms
Figure
-

Fig. 1 Three-dimensional measurements of right atrial (A), left atrial (B), and left atrial appendage (C) volumes using software (Aquaris Intuition Edition V4.4.6, TeraRecon, San Francisco, CA, USA) on multidetector computed tomography images.

Fig. 2 Strong linear correlation between the right atrial and left atrial volume indices in patients with/without early recurrence (A) and in patients with/without 1-year recurrence (B). RAVI: right atrial volume indices, LAVI: left atrial volume indices.
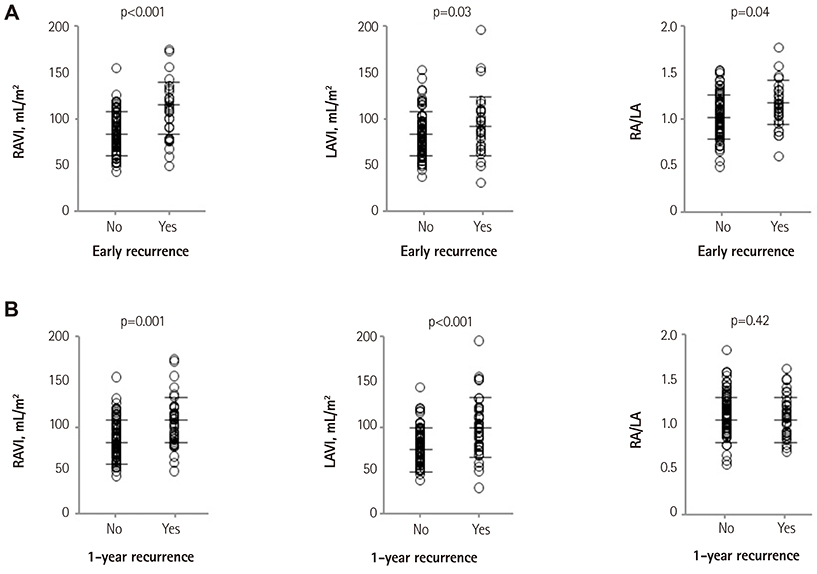
Fig. 3 Comparisons of both atrial volume indices and the ratio of right atrial (RA) volume to left atrial (LA) size between patients with/without early (A) or 1-year recurrence (B). Note that RA/LA is significantly higher in the early recurrence group, but not in the 1-year recurrence group. RAVI: right atrial volume indices, LAVI: left atrial volume indices.
Cited by 2 articles
-
The Impact of Right Atrial Size to Predict Success of Direct Current Cardioversion in Patients With Persistent Atrial Fibrillation
Christoph Döring, Utz Richter, Stefan Ulbrich, Carsten Wunderlich, Micaela Ebert, Sergio Richter, Axel Linke, Krunoslav Michael Sveric
Korean Circ J. 2023;53(5):331-343. doi: 10.4070/kcj.2022.0291.Is Right Atrial Remodeling an Additional Marker for the Progression of Atrial Fibrillation?
Jin-Kyu Park
Korean Circ J. 2023;53(5):344-346. doi: 10.4070/kcj.2023.0069.
Reference
-
1. Heeringa J, van der Kuip DA, Hofman A, et al. Prevalence, incidence and lifetime risk of atrial fibrillation: the Rotterdam study. Eur Heart J. 2006; 27:949–953.2. Wann LS, Curtis AB, January CT, et al. 2011 ACCF/AHA/HRS focused update on the management of patients with atrial fibrillation (updating the 2006 guideline): a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation. 2011; 123:104–123.3. Wijffels MC, Kirchhof CJ, Dorland R, Allessie MA. Atrial fibrillation begets atrial fibrillation. A study in awake chronically instrumented goats. Circulation. 1995; 92:1954–1968.4. Ausma J, Wijffels M, Thoné F, Wouters L, Allessie M, Borgers M. Structural changes of atrial myocardium due to sustained atrial fibrillation in the goat. Circulation. 1997; 96:3157–3163.5. Allessie M, Ausma J, Schotten U. Electrical, contractile and structural remodeling during atrial fibrillation. Cardiovasc Res. 2002; 54:230–246.6. Avitall B, Bi J, Mykytsey A, Chicos A. Atrial and ventricular fibrosis induced by atrial fibrillation: evidence to support early rhythm control. Heart Rhythm. 2008; 5:839–845.7. Schoonderwoerd BA, Ausma J, Crijns HJ, Van Veldhuisen DJ, Blaauw EH, Van Gelder IC. Atrial ultrastructural changes during experimental atrial tachycardia depend on high ventricular rate. J Cardiovasc Electrophysiol. 2004; 15:1167–1174.8. Hu YF, Chen YJ, Lin YJ, Chen SA. Inflammation and the pathogenesis of atrial fibrillation. Nat Rev Cardiol. 2015; 12:230–243.9. Li D, Fareh S, Leung TK, Nattel S. Promotion of atrial fibrillation by heart failure in dogs: atrial remodeling of a different sort. Circulation. 1999; 100:87–95.10. Bauer A, McDonald AD, Donahue JK. Pathophysiological findings in a model of persistent atrial fibrillation and severe congestive heart failure. Cardiovasc Res. 2004; 61:764–770.11. Lang RM, Bierig M, Devereux RB, et al. Recommendations for chamber quantification: a report from the American Society of Echocardiography's Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J Am Soc Echocardiogr. 2005; 18:1440–1463.12. Sanfilippo AJ, Abascal VM, Sheehan M, et al. Atrial enlargement as a consequence of atrial fibrillation. A prospective echocardiographic study. Circulation. 1990; 82:792–797.13. Schotten U, Ausma J, Stellbrink C, et al. Cellular mechanisms of depressed atrial contractility in patients with chronic atrial fibrillation. Circulation. 2001; 103:691–698.14. Luong C, Thompson DJ, Bennett M, et al. Right atrial volume is superior to left atrial volume for prediction of atrial fibrillation recurrence after direct current cardioversion. Can J Cardiol. 2015; 31:29–35.15. O'Neill MD, Jaïs P, Takahashi Y, et al. The stepwise ablation approach for chronic atrial fibrillation--evidence for a cumulative effect. J Interv Card Electrophysiol. 2006; 16:153–167.16. Andrade JG, Khairy P, Verma A, et al. Early recurrence of atrial tachyarrhythmias following radiofrequency catheter ablation of atrial fibrillation. Pacing Clin Electrophysiol. 2012; 35:106–116.17. European Heart Rhythm Association (EHRA). European Cardiac Arrhythmia Scoiety (ECAS). American College of Cardiology (ACC). . HRS/EHRA/ECAS expert Consensus Statement on catheter and surgical ablation of atrial fibrillation: recommendations for personnel, policy, procedures and follow-up. A report of the Heart Rhythm Society (HRS) Task Force on catheter and surgical ablation of atrial fibrillation. Heart Rhythm. 2007; 4:816–861.18. O'Donnell D, Furniss SS, Dunuwille A, Bourke JP. Delayed cure despite early recurrence after pulmonary vein isolation for atrial fibrillation. Am J Cardiol. 2003; 91:83–85.19. Moon J, Hong YJ, Shim J, et al. Right atrial anatomical remodeling affects early outcomes of nonvalvular atrial fibrillation after radiofrequency ablation. Circ J. 2012; 76:860–867.20. Arya A, Hindricks G, Sommer P, et al. Long-term results and the predictors of outcome of catheter ablation of atrial fibrillation using steerable sheath catheter navigation after single procedure in 674 patients. Europace. 2010; 12:173–180.21. Jiang H, Lu Z, Lei H, Zhao D, Yang B, Huang C. Predictors of early recurrence and delayed cure after segmental pulmonary vein isolation for paroxysmal atrial fibrillation without structural heart disease. J Interv Card Electrophysiol. 2006; 15:157–163.22. Lee SH, Tai CT, Hsieh MH, et al. Predictors of early and late recurrence of atrial fibrillation after catheter ablation of paroxysmal atrial fibrillation. J Interv Card Electrophysiol. 2004; 10:221–226.23. Themistoclakis S, Schweikert RA, Saliba WI, et al. Clinical predictors and relationship between early and late atrial tachyarrhythmias after pulmonary vein antrum isolation. Heart Rhythm. 2008; 5:679–685.24. Bhargava M, Di Biase L, Mohanty P, et al. Impact of type of atrial fibrillation and repeat catheter ablation on long-term freedom from atrial fibrillation: results from a multicenter study. Heart Rhythm. 2009; 6:1403–1412.25. Verma A, Wazni OM, Marrouche NF, et al. Pre-existent left atrial scarring in patients undergoing pulmonary vein antrum isolation: an independent predictor of procedural failure. J Am Coll Cardiol. 2005; 45:285–292.26. Pappone C, Santinelli V, Manguso F, et al. Pulmonary vein denervation enhances long-term benefit after circumferential ablation for paroxysmal atrial fibrillation. Circulation. 2004; 109:327–334.27. Hof IE, Velthuis BK, Chaldoupi SM, et al. Pulmonary vein antrum isolation leads to a significant decrease of left atrial size. Europace. 2011; 13:371–375.28. Akutsu Y, Kaneko K, Kodama Y, et al. Association between left and right atrial remodeling with atrial fibrillation recurrence after pulmonary vein catheter ablation in patients with paroxysmal atrial fibrillation: a pilot study. Circ Cardiovasc Imaging. 2011; 4:524–531.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Chronic Radiodermatitis following Radiofrequency Catheter Ablation for Atrial Fibrillation
- A Case of Successful Ablation of Right-Sided Accessory Pathway during Atrial Fibrillation
- Radiofrequency Catheter Ablation of Persistent Atrial Fibrillation with Myotonic Dystrophy and Achalasia-like Esophageal Dilatation
- Cerebral Infarction After Radiofrequency Catheter Ablation in Patients With Paroxysmal Atrial Fibrillation
- The Mechanism of and Preventive Therapy for Stroke in Patients with Atrial Fibrillation
