Cerebrospinal Fluid Rhinorrhea and Seizure Caused by Temporo-Sphenoidal Encephalocele
- Affiliations
-
- 1Department of Neurosurgery, Klinikum Nurnberg, Paracelsus Medical University, Nurnberg, Germany. alexander.hammer@klinikum-nuernberg.de
- 2Institute of Radiology and Neuroradiology, Klinikum Nurnberg, Paracelsus Medical University, Nurnberg, Germany.
- 3Department of Neurosurgery, University of Heidelberg, Heidelberg, Germany.
- KMID: 1956431
- DOI: http://doi.org/10.3340/jkns.2015.57.4.298
Abstract
- This case report describes the symptoms and clinical course of a 35-year-old female patient who was diagnosed with a temporo-sphenoidal encephalocele. It is characterized by herniation of cerebral tissue of the temporal lobe through a defect of the skull base localized in the middle fossa. At the time of first presentation the patient complained about recurrent nasal discharge of clear fluid which had begun some weeks earlier. She also reported that three months earlier she had for the first time suffered from a generalized seizure. In a first therapeutic attempt an endoscopic endonasal approach to the sphenoid sinus was performed. An attempt to randomly seal the suspicious area failed. After frontotemporal craniotomy, it was possible to localize the encephalocele and the underlying bone defect. The herniated brain tissue was resected and the dural defect was closed with fascia of the temporalis muscle. In summary, the combination of recurrent rhinorrhea and a first-time seizure should alert specialists of otolaryngology, neurology and neurosurgery of a temporo-sphenoidal encephalocele as a possible cause. Treatment is likely to require a neurosurgical approach.
MeSH Terms
Figure
-
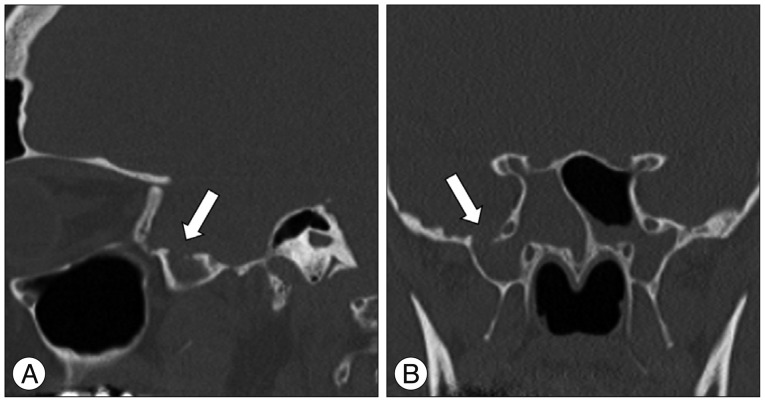
Fig. 1 Sagittal (A) and coronal (B) computed tomography scan of the skull base showing the defect (6.2×6.3×7.2 mm) in the roof of a far lateral recessus of the right sphenoid sinus leading to the middle fossa (arrows).
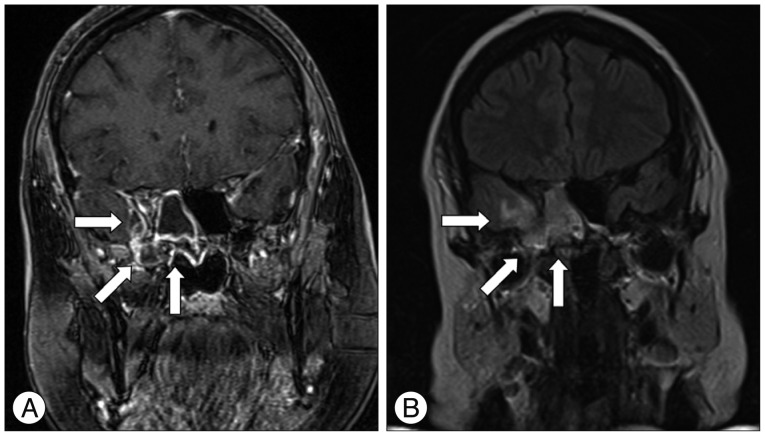
Fig. 2 A : Coronal T1-weighted magnetic resonance imaging scan of the head showing a disruption of the skull base in the area of the roof of the right sphenoid sinus where the encephalocele penetrated. A contrast enhancement in terms of an inflammatory area reaching to the fronto-mesial temporal lobe is detectable (arrows). B : Coronal T2-weighted/FLAIR magnetic resonance imaging scan of the head showing a high signal intensity of the right temporal lobe reconcilable with an encephalitis (arrows). FLAIR : fluid attenuated inversion recovery.

Fig. 3 A : The middle cranial fossa is reached via a fronto-temporal approach. This way, the damaged dura and skull base become visible (arrows). B : Upon resection of the encephalocele, the dura defect is sealed with galea, tachosil, and fibrin glue (arrow).

Fig. 4 A : Coronal T1-weighted magnetic resonance imaging scan of the head showing no contrast enhancement in terms of an inflammatory area of the fronto-mesial temporal lobe (arrows). B : Coronal T2-weighted/FLAIR magnetic resonance imaging scan of the head. No abnormal signal intensity are detected in the area of the right temporal lobe (arrows). FLAIR : fluid attenuated inversion recovery.
Cited by 1 articles
-
A Case of Sphenoidal Meningoencephalocele Masquerading as an Isolated Sphenoid Mucocele
Young-Chan Kim, Jiwon Kwak, Hyeongeun Kim, Sang Hag Lee
Korean J Otorhinolaryngol-Head Neck Surg. 2021;64(9):680-683. doi: 10.3342/kjorl-hns.2021.00290.
Reference
-
1. Acherman DS, Bosman DK, van der Horst CM. Sphenoethmoidal encephalocele : a case report. Cleft Palate Craniofac J. 2003; 40:329–333. PMID: 12733965.2. Arai A, Mizukawa K, Nishihara M, Fujita A, Hosoda K, Kohmura E. Spontaneous cerebrospinal fluid rhinorrhea associated with a far lateral temporal encephalocele--case report. Neurol Med Chir (Tokyo). 2010; 50:243–245. PMID: 20339278.
Article3. Barañano CF, Curé J, Palmer JN, Woodworth BA. Sternberg's canal : fact or fiction? Am J Rhinol Allergy. 2009; 23:167–171. PMID: 19401043.4. Buchfelder M, Fahlbusch R, Huk WJ, Thierauf P. Intrasphenoidal encephaloceles--a clinical entity. Acta Neurochir (Wien). 1987; 89:10–15. PMID: 3324649.
Article5. Catala M. [Embryology of the sphenoid bone]. J Neuroradiol. 2003; 30:196–200. PMID: 14566186.6. Elster AD, Branch CL Jr. Transalar sphenoidal encephaloceles : clinical and radiologic findings. Radiology. 1989; 170(1 Pt 1):245–247. PMID: 2909104.
Article7. Friedman A, Dingledine R. Molecular cascades that mediate the influence of inflammation on epilepsy. Epilepsia. 2011; 52(Suppl 3):33–39. PMID: 21542844.
Article8. Hwang K, Kim HJ. Congenital orbital encephalocele, orbital dystopia, and exophthalmos. J Craniofac Surg. 2012; 23:e343–e344. PMID: 22801176.
Article9. Kaufman B, Yonas H, White RJ, Miller CF 2nd. Acquired middle cranial fossa fistulas : normal pressure and nontraumatic in origin. Neurosurgery. 1979; 5:466–472. PMID: 534052.10. Kumar R, Jenkins A. Spontaneous CSF rhinorrhoea due to temporosphenoidal encephalocele. Br J Neurosurg. 1998; 12:66–68. PMID: 11013655.
Article11. Kwon JE, Kim E. Middle fossa approach to a temporosphenoidal encephalocele -technical note-. Neurol Med Chir (Tokyo). 2010; 50:434–438. PMID: 20505307.
Article12. Lai SY, Kennedy DW, Bolger WE. Sphenoid encephaloceles : disease management and identification of lesions within the lateral recess of the sphenoid sinus. Laryngoscope. 2002; 112:1800–1805. PMID: 12368619.
Article13. Landreneau FE, Mickey B, Coimbra C. Surgical treatment of cerebrospinal fluid fistulae involving lateral extension of the sphenoid sinus. Neurosurgery. 1998; 42:1101–1104. discussion 1104-1105. PMID: 9588555.
Article14. Lesavoy MA, Nguyen DT, Yospur G, Dickinson BP. Nasopharyngeal encephalocele : report of transcranial and transpalatal repair with a 25-year follow-up. J Craniofac Surg. 2009; 20:2251–2256. PMID: 19934685.15. Matsumoto M, Akati K, Hashimoto T, Nakamura N. [Basal encephalomeningocele occurring in an aged woman; a case report and the usefulness of MRI in diagnosis]. No Shinkei Geka. 1992; 20:157–159. PMID: 1542394.16. Mikami T, Saito K, Okuyama T, Sakamoto Y, Takahashi A, Shibata K. [A case of transethmoidal meningocele showing increased activity of 99mTcHM-PAO at seizure attack]. No To Shinkei. 1998; 50:63–67. PMID: 9493201.17. Papanikolaou V, Bibas A, Ferekidis E, Anagnostopoulou S, Xenellis J. Idiopathic temporal bone encephalocele. Skull Base. 2007; 17:311–316. PMID: 18330429.
Article18. Rivierez M, Valsaint P. [Spontaneous temporo-sphenoidal encephalocele. A case report]. Neurochirurgie. 2000; 46:383–386. PMID: 11015676.19. Shimizu T, Kitamura S, Kinouchi K, Fukumitsu K. A rare case of upper airway obstruction in an infant caused by basal encephalocele complicating facial midline deformity. Paediatr Anaesth. 1999; 9:73–76. PMID: 10712719.
Article20. Soyer P, Dobbelaere P, Reizine D, Ferquel C. Transalar sphenoidal meningoencephalocele associated with buccal angiomatosis. One case. J Neuroradiol. 1990; 17:222–226. PMID: 2286845.21. Suwanwela C, Suwanwela N. A morphological classification of sincipital encephalomeningoceles. J Neurosurg. 1972; 36:201–211. PMID: 5008734.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endoscope-Assisted Trans-Sphenoidal Approach for Treatment of Sternberg's Canal
- Traumatic Cerebrospinal Fluid Rhinorrhea: Successful Closure under the Surgical Microscope
- A Case of Empty Sella Syndrome with Cerebrospinal Fluid Rhinorrhea
- Endoscopic treatment of iatrogenic cerebrospinal fluid rhinorrhea
- Bacterial Meningitis and Cerebrospinal Fluid Rhinorrhea Related to Rhinoplasty
