The Posterior Fixation of Thoracolumbar Burst Fracture using Pedicle Screws and Caudal Offset Sublaminar Hooks
- Affiliations
-
- 1Department of Orthopedic Surgery, Soonchunhyang University College of Medicine, Bucheon, Korea.
- 2Department of Orthopedic Surgery, National Medical Center, Seoul, Korea. ljhos@medimail.co.kr
- KMID: 1897019
- DOI: http://doi.org/10.4184/jkss.2005.12.1.39
Abstract
- STUDY DESIGN: A retrospective study.
OBJECTIVES
We analyzed the clinical results of thoracolumbar burst fractures, managed by posterior fixation of 2 segments above and 1 segment below, using an offset sublaminar hook. SUMMARY OF LITERATURE REVIEW: Mono-segment fixation above and below the injured vertebra, using posterior pedicle screw fixation, has the benefit of saving the uninjured mobile lumbar segment in thoracolumbar junction burst fracture patients. However, in a severely comminuted vertebral body, mono-segment fixation may not prevent loss of correction and metal failure. Options for such cases are additional anterior column support or long segment fixation, including 2 segments above and 1 below the injured vertebra. Instead of fixing 2 segments below the fracture level, fixation of one segment below, using the offset sublaminar hook, can save the uninjured segment, especially in the upper lumbar segment, with greater fixation strength than mono-segmental screws only. MATERIAL AND METHOD: The study included eleven patients with a thoracolumbar junction burst fracture, which underwent posterior fixation using pedicle screws in 2 segments above and 1 segment below, aided by an offset sublaminar hook. The mean follow-up period was 30.7 months (range, 24 to 58 months). Radiographs taken at follow-up were evaluated for implant loosening, correction loss, change in pedicle screw angle, and loss of vertebral height, adjacent segment instability and junctional degenerative change. The clinical results were collected in out-patient department.
RESULTS
No implant loosening was noted. No case showed adjacent instability, acceleration of junctional degenerative change at the lower end of lumbar segment or hook dislodgement. Also, there were no junctional area related symptoms.
CONCLUSION
For posterior surgery of thoracolumbar burst fractures, this construct, fixing 2 segments above and 1 segment below injured vertebra, aided by an offset sublaminar hook, was satisfactory in maintaining fracture reduction, and showed no instability or acceleration of degeneration on adjacent segnents.
Figure
-
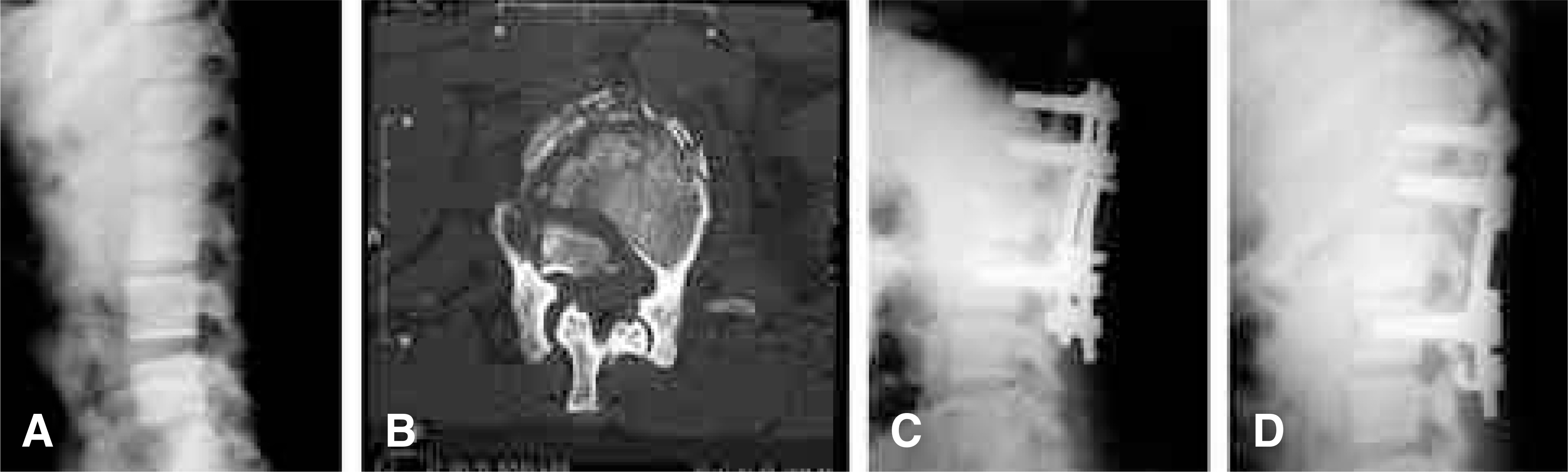
Fig. 1. (A) Radiographs showing initial findings. Initial radiograph shows burst fracture of L2 vertebral body with severe kyphotic deformity. (B) Initial CT scan shows gross comminution of vertebral body. Load sharing classification score was 9. (C) Radiographs showing immediate postop findings. Immediate postop radiographs show nearly complete reduction of L2 vertebral body with restoration of normal vertebral body height. (D) Radiographs showing 24 months followup findings. 24 months followup radiographs show well maintained reduction and vertebral body height. Clinically, patient showed no mid or lower back pain.
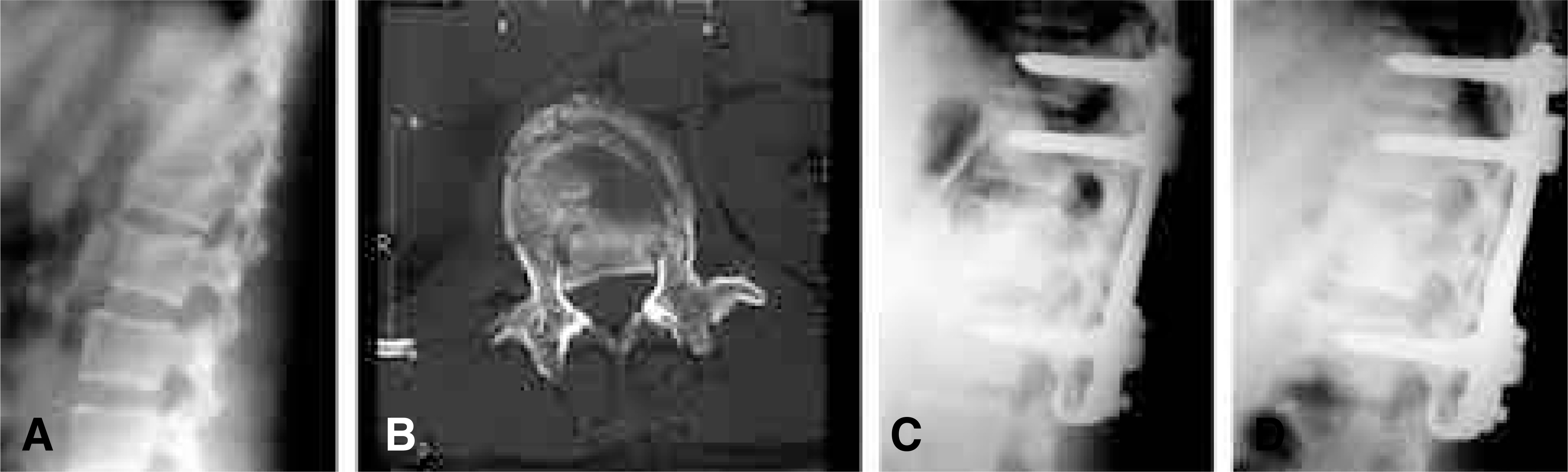
Fig. 2. (A) Radiographs showing initial findings. Initial radiograph shows burst fracture of L1 vertebral body with severe kyphotic deformity. (B) Initial CT scan shows gross comminution of vertebral body. Load sharing classification score was 8. (C) Radiographs showing immediate postop findings. Immediate postop radiograph shows nearly complete reduction of L1 vertebral body with restoration of normal vertebral body height. (D) Radiographs showing 28 months followup findings. 28 months followup radiograph shows well maintained reduction and vertebral body height.
Reference
-
1). Dewald RL. Burst fractures of the thoracic and lumbar spine. Clin Orthop. 1984; 189:150–161.
Article2). Esses SI, Botsford DJ, Wright T, Bednar D, Bailey S. Operative treatment of spinal fractures with the AO internal fixator. Spine. 1991; 16:146–150.
Article3). Garfin SR, Mowery CA, Guerra J, Marshall LF. Confirmation of the posterolateral technique to decompress and fuse thoracolumbar spine burst fractures. Spine. 1985; 10:218–223.
Article4). McBride GG. Cotrel-Dubousset rods in surgical stabilization of spinal fractures. Spine. 1993; 18:466–473.
Article5). Stambough JL. Cotrel-Dubousset instrumentation and thoracolumbar spine trauma: A review of 55 cases. J Spinal Disord. 1994; 7:462–469.6). Zindrick MR. The role of transpedicular fixation system for stabilization of the lumbar spine. Orthop Clin North Am. 1991; 22:333–344.7). McCormack T, Karaikovic E, Gaines RW. The load sharing classification of spinal fractures. Spine. 1994; 19:1741–1744.8). Dickson JH, Harrington PR, Erwin WD. Results of reduction and stabilization of the severely fractured thoracic and lumbar spine. J Bone Joint Surg. 1978; 60:799–805.
Article9). Wang JM, Roh KJ, Kim DJ, Kim DW, Yun YH, Kim SW. Long segment pedicle instrumentation and anterior interbody fusion for thoraclumbar burst fractures. J Kor Orthop Assoc. 1994; 29:1672–1678.
Article10). Roy-Camille R, Benazet JP, Desauge JP, Kuntz F. Lumbosacral fusion with pedicluar screw plating instrumentation: A 10-year followup. Acta Orthop Scand. 1993; 251:100–104.11). Roy-Camille R, Saillant G, Beraux D, Salgado V. Osteosynthesis of thoracolumbar spine fractures with metal plates screwed through the vertebral pedicles. Reconstr Surg Traumatol. 1976; 15:2–16.12). Roy-Camille R, Saillant G, Mazel CH. Plating of thoracic, thoracolumbar, and lumbar injuries with pedicle screw plates. Orthop Clin North Am. 1986; 17:147–159.
Article13). McLain RF, Sparling E, Benson DR. Early failure of short-segment pedicle instrumentation for thoracolumbar fractures. J Bone Joint Surg. 1993; 75:162–167.14). Chung YK, Kim SW. Short - and long - segment pedicle screw fixation with anterior interbody fusion with short bone graft in Denis type B burst fractures. J Kor Spine Surg. 1998; 5:159–168.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Short Segment versus Long Segment Pedicle Screws Fixation in Management of Thoracolumbar Burst Fractures: Meta-Analysis
- Surgical Management of Thoracolumbar Spine Fracture with Pedicle Screws and Inferior Laminar Hooks
- Long Segmental Fixation for unstable Thoracolumbar Fracture Without Severe Neurologic Involvement
- One Stage Decompression and Circumferential Stabilization by Posterior Approach in the Unstable Burst Fracture of Thoracolumbar and Lumbar Spine
- Pedicle Screw Fixation in the Treatment of Unstable Thoracolumbar and Lumbar Fracture
