Korean J Urol.
2014 Jun;55(6):411-416. 10.4111/kju.2014.55.6.411.
Effect of Potassium Magnesium Citrate and Vitamin B-6 Prophylaxis for Recurrent and Multiple Calcium Oxalate and Phosphate Urolithiasis
- Affiliations
-
- 1Department of Urology, Narayana Medical College and Hospital, Nellore, India. vijaya.nel@gmail.com
- 2Department of Community Medicine and Biostatistics, Narayana Medical College and Hospital, Nellore, India.
- 3Department of Biochemistry, Narayana Medical College and Hospital, Nellore, India.
- KMID: 1885621
- DOI: http://doi.org/10.4111/kju.2014.55.6.411
Abstract
- PURPOSE
To study the effects of long-term treatment with potassium magnesium citrate and vitamin B-6 prophylaxis (Urikind-KM6; 1,100-mg potassium citrate, 375-mg magnesium citrate, and 20-mg pyridoxine hydrochloride/5 mL) every 8 hours over 3 years.
MATERIALS AND METHODS
A total of 247 patients with recurrent idiopathic hypocitraturia with or without hyperuricosuria and randomized controls were studied prospectively for 3 years. The total patients were divided into three groups. Control group 1 consisted of 61 patients (24.7%) who had moderate to severe hypocitraturia with or without hyperuricosuria and were recurrent stone formers but discontinued prophylaxis because of drug intolerance within 1 month of therapy. Control group 2 constituted 53 patients (21.5%) who were first-time stone formers and who had mild hypocitraturia with or without hyperuricosuria and were not put on prophylactic therapy and were followed for 3.16+/-0.08 years. Control group 3 constituted 133 patients (54.8%) who were recurrent stone formers who had moderate to severe hypocitraturia with or without hyperuricosuria and were put on prophylaxis therapy and were followed for 3.16+/-0.08 years. All patients were followed up at 6-month intervals.
RESULTS
Potassium magnesium citrate prophylaxis produced a sustained increase in 24-hour urinary citrate excretion from initially low values (221.79+/-13.39 mg/dL) to within normal to high limits (604.04+/-5.00 mg/dL) at the 6-month follow-up. Urinary pH rose significantly from 5.62+/-0.2 to 6.87+/-0.01 and was maintained at 6.87+/-0.01. The stone recurrence rate declined from 3.23+/-1.04 per patient per year to 0.35+/-0.47 per patient per year.
CONCLUSIONS
Potassium magnesium citrate prophylaxis was effective in reducing the recurrence of calcium oxalate and phosphate urolithiasis.
MeSH Terms
Figure
-
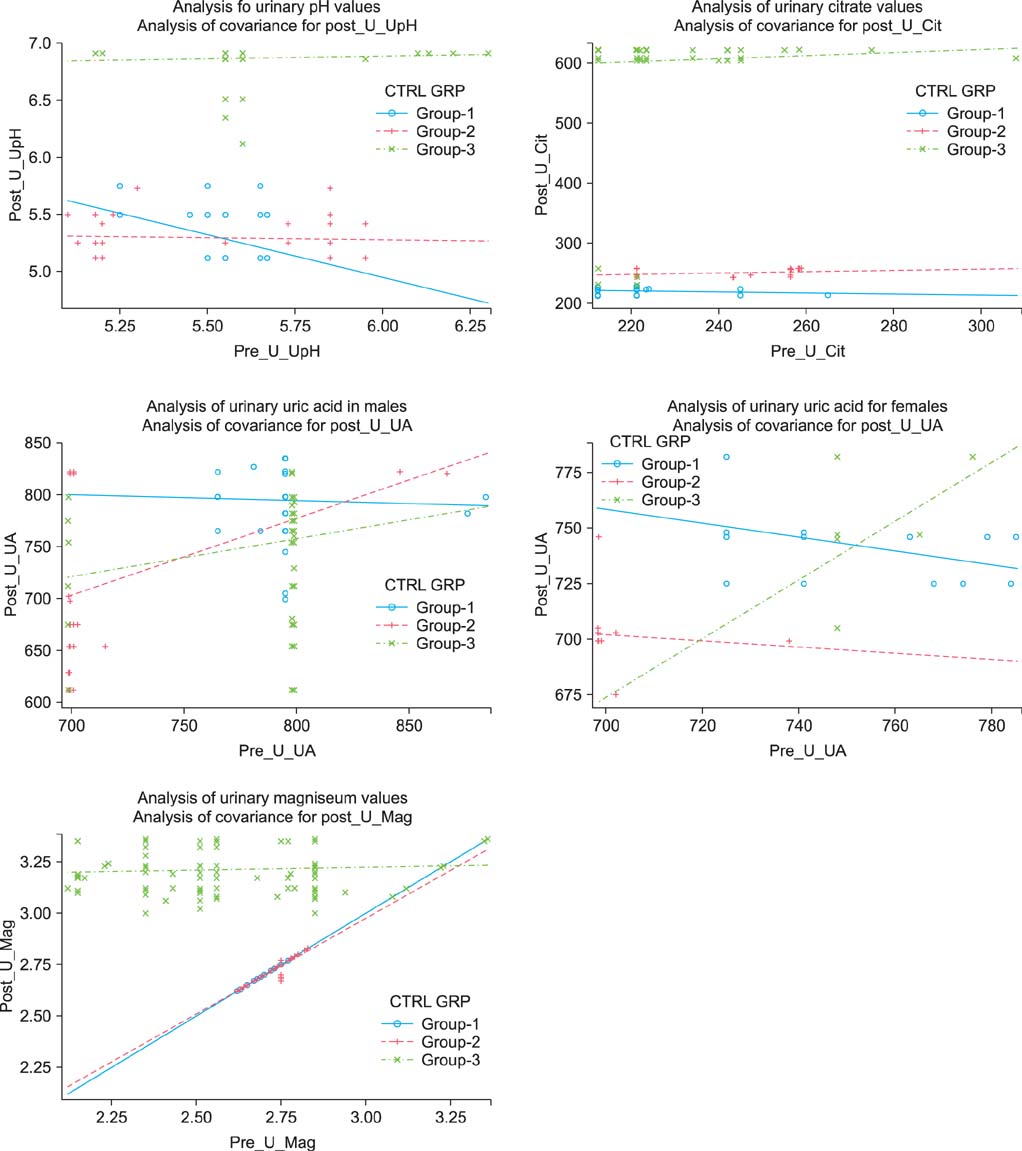
FIG. 1 Comparitive analysis of pre- and posttreatment urinary values.
Reference
-
1. Ramello A, Vitale C, Marangella M. Epidemiology of nephrolithiasis. J Nephrol. 2000; 13:Suppl 3. S45–S50.2. Turney BW, Reynard JM, Noble JG, Keoghane SR. Trends in urological stone disease. BJU Int. 2012; 109:1082–1087.3. Ljunghall S, Danielson BG. A prospective study of renal stone recurrences. Br J Urol. 1984; 56:122–124.4. Shetty PS. Nutrition transition in India. Public Health Nutr. 2002; 5(1A):175–182.5. Taylor EN, Curhan GC. Fructose consumption and the risk of kidney stones. Kidney Int. 2008; 73:207–212.6. Meschi T, Maggiore U, Fiaccadori E, Schianchi T, Bosi S, Adorni G, et al. The effect of fruits and vegetables on urinary stone risk factors. Kidney Int. 2004; 66:2402–2410.7. Taylor EN, Curhan GC. Oxalate intake and the risk for nephrolithiasis. J Am Soc Nephrol. 2007; 18:2198–2204.8. Koyuncu HH, Yencilek F, Eryildirim B, Sarica K. Family history in stone disease: how important is it for the onset of the disease and the incidence of recurrence? Urol Res. 2010; 38:105–109.9. Curhan GC, Willett WC, Rimm EB, Stampfer MJ. Family history and risk of kidney stones. J Am Soc Nephrol. 1997; 8:1568–1573.10. D'Angelo A, Calo L, Cantaro S, Giannini S. Calciotropic hormones and nephrolithiasis. Miner Electrolyte Metab. 1997; 23:269–272.11. Paliouras C, Trampikaki E, Alirasis P, Aperis G. Pathophysiology of nephrolithiasis. Nephrol Rev. 2012; 4:e14.12. Johri N, Cooper B, Robertson W, Choong S, Rickards D, Unwin R. An update and practical guide to renal stone management. Nephron Clin Pract. 2010; 116:c159–c171.13. Hamm LL, Hering-Smith KS. Pathophysiology of hypocitraturic nephrolithiasis. Endocrinol Metab Clin North Am. 2002; 31:885–893.14. Domrongkitchaiporn S, Stitchantrakul W, Kochakarn W. Causes of hypocitraturia in recurrent calcium stone formers: focusing on urinary potassium excretion. Am J Kidney Dis. 2006; 48:546–554.15. Welch BJ, Graybeal D, Moe OW, Maalouf NM, Sakhaee K. Biochemical and stone-risk profiles with topiramate treatment. Am J Kidney Dis. 2006; 48:555–563.16. Melnick JZ, Preisig PA, Haynes S, Pak CY, Sakhaee K, Alpern RJ. Converting enzyme inhibition causes hypocitraturia independent of acidosis or hypokalemia. Kidney Int. 1998; 54:1670–1674.17. Amanzadeh J, Gitomer WL, Zerwekh JE, Preisig PA, Moe OW, Pak CY, et al. Effect of high protein diet on stone-forming propensity and bone loss in rats. Kidney Int. 2003; 64:2142–2149.18. Marangella M, Vitale C, Manganaro M, Cosseddu D, Martini C, Petrarulo M, et al. Renal handling of citrate in chronic renal insufficiency. Nephron. 1991; 57:439–443.19. Weinstein DA, Somers MJ, Wolfsdorf JI. Decreased urinary citrate excretion in type 1a glycogen storage disease. J Pediatr. 2001; 138:378–382.20. Pak CY. Physicochemical basis for formation of renal stones of calcium phosphate origin: calculation of the degree of saturation of urine with respect to brushite. J Clin Invest. 1969; 48:1914–1922.21. Pak CY, Sakhaee K, Peterson RD, Poindexter JR, Frawley WH. Biochemical profile of idiopathic uric acid nephrolithiasis. Kidney Int. 2001; 60:757–761.22. Pak CY. Citrate and renal calculi: an update. Miner Electrolyte Metab. 1994; 20:371–377.23. Lee SY, Moon YT. Clinical significance of hypocitraturia in patients with nephrolithiasis. Korean J Urol. 2006; 47:631–634.24. Kok DJ, Papapoulos SE, Bijvoet OL. Excessive crystal agglomeration with low citrate excretion in recurrent stone-formers. Lancet. 1986; 1:1056–1058.25. Tiselius HG. The effect of pH on the urinary inhibition of calcium oxalate crystal growth. Br J Urol. 1981; 53:470–474.26. Hosking DH, Erickson SB, Van den Berg CJ, Wilson DM, Smith LH. The stone clinic effect in patients with idiopathic calcium urolithiasis. J Urol. 1983; 130:1115–1118.27. Pak CY, Peterson R. Successful treatment of hyperuricosuric calcium oxalate nephrolithiasis with potassium citrate. Arch Intern Med. 1986; 146:863–867.28. Ettinger B, Pak CY, Citron JT, Thomas C, Adams-Huet B, Vangessel A. Potassium-magnesium citrate is an effective prophylaxis against recurrent calcium oxalate nephrolithiasis. J Urol. 1997; 158:2069–2073.29. Jaipakdee S, Prasongwatana V, Premgamone A, Reungjui S, Tosukhowong P, Tungsanga K, et al. The effects of potassium and magnesium supplementations on urinary risk factors of renal stone patients. J Med Assoc Thai. 2004; 87:255–263.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Infrared Spectroscopy Analysis of the Urinary Calculi of Korean People
- Calcium Oxalate and Calcium Phosphate Crystal Formation and Inhibition in Agarose Gel System
- Change of 24-hour Urinary Citrate Level after Dietary Manipulation with Lemon Juice in Urolithiasis Patients
- Management of Urinary Stone with Potassium Citrate
- Effects of Oral Administration of Citrate, Thiazide, Allopurinol and Magnesium on Renal Calcium Oxalate Crystal Formation and Osteopontin Expression in a Rat Urolithiasis Model
