Pulmonary Coccidioidomycosis in Immunocompetent Patient
- Affiliations
-
- 1Department of Internal Medicine, University of Dongguk College of Medicine, Dongguk University Ilsan Hospital, Goyang, Korea. pgm1134@duih.org
- 2Department of Pathology, University of Dongguk College of Medicine, Dongguk University Ilsan Hospital, Goyang, Korea.
- KMID: 1846384
- DOI: http://doi.org/10.4046/trd.2009.66.3.220
Abstract
- Coccidioidomycosis is a fungal infection caused by the soil fungus, Coccidioides immitis, which is endemic to the south-western United States. However, the incidence of coccidioidomycosis has recently increased due to the increase in overseas travel to endemic areas. We report a case of pulmonary coccidioidomycosis diagnosed in an immunocompetent person. A 28-year-old female, who had lived in Phoenix, Arizona, USA for 2 years, was admitted for an evaluation of persistent cough with fever lasting for 2 weeks. The chest X-ray and Chest CT revealed multifocal patchy consolidation and ground-glass opacity in both lungs as well as multiple enlarged right hilar and paratracheal lymph nodes. A percutaneous needLe biopsy of the main mass-like consolidation confirmed mature spherules of Coccidioides immitis in lung tissue. Pulmonary coccidioidomycosis should be considered in patients presenting with persistent cough with fever and a history of travel to or immigration from an endemic area.
Keyword
MeSH Terms
Figure
-
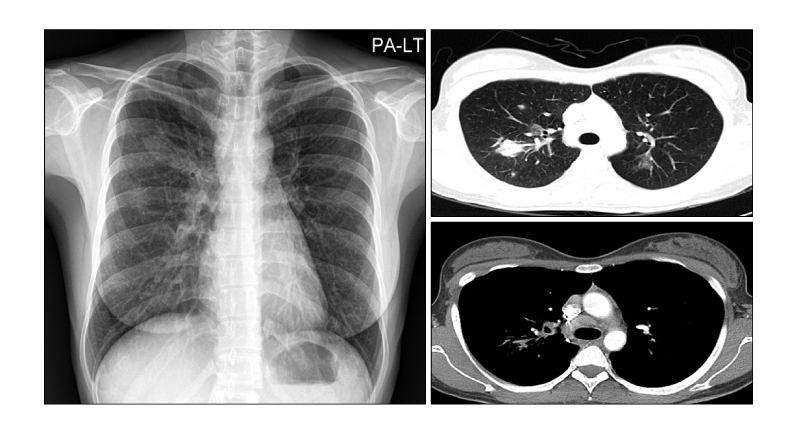
Figure 1 Chest PA and Chest CT on the admission day show multifocal patchy consolidation and ground-glass opacity (GGO) in RUL, GGO in LUL and mediastinal lymph node enlargement.
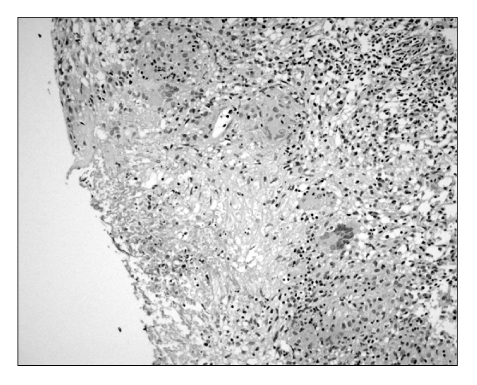
Figure 2 Microscopic finding shows multiple scattered granulomas with central necrosis (H&E stain, ×200).
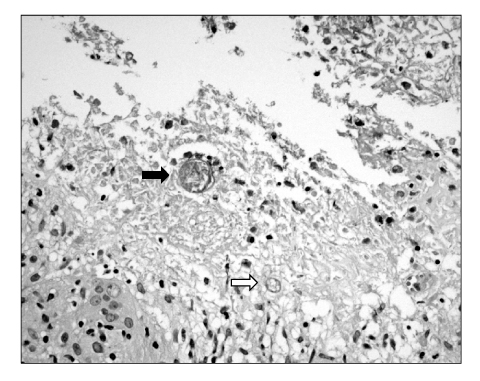
Figure 3 Microscopic finding shows immature spherule (white arrow) and mature spherule (black arrow). Mature spherules contain degenerated endospores (H&E stain, ×400).
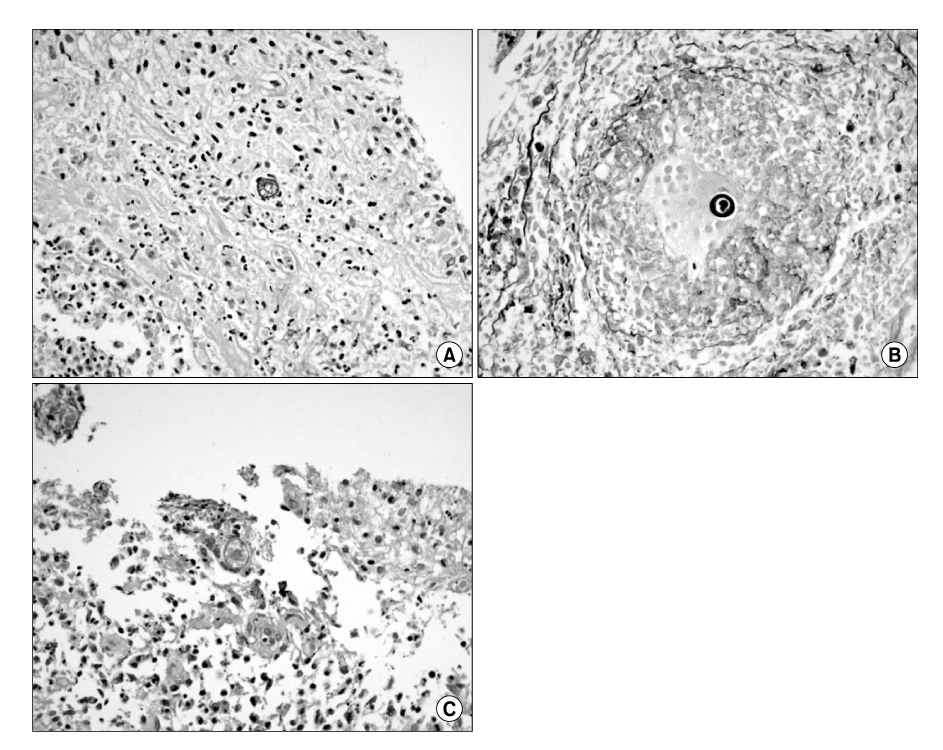
Figure 4 The walls and contents of spherules are PAS positive (A), GMS positive (B) and mucicarmine negative (C).
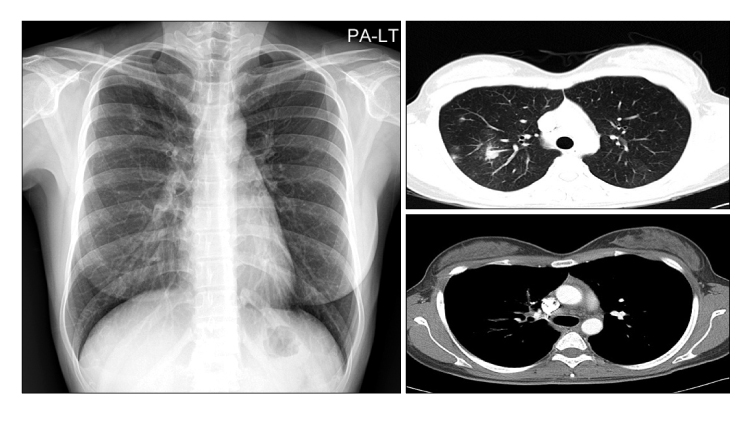
Figure 5 Chest PA and Chest CT on the post-fluconazole treatment day 14 show decreased consolidation in RUL, disappeared ground-glass opacity (GGO) in LUL and improved mediastinal lymph node enlargement.
Cited by 1 articles
-
A Case of Coccidioidal Meningitis
Jung Woo Lee, Sang Il Kim, Youn Jeong Kim, Jae-Cheol Kwon, Ye Jee Lim, Mi Hee Park, Seon A Kim, Eun Sil Koh, Min Ju Kim, Moon Won Kang
Infect Chemother. 2012;44(2):75-79. doi: 10.3947/ic.2012.44.2.75.
Reference
-
1. Kim JH, Kim MA, Yang SK, Choi TY, Kim CW, Kim KH. A case of coccidioidomycosis. Korean J Dermatol. 1976. 14:73–79.2. Woo JH, Lee JS, Lee DW, Jin SY, Kim DW, Lee WG. A case of disseminated coccidioidomycosis. J Korean Med Sci. 1996. 11:258–264.3. Han SY, Kim CH, Son KP, Kim JK, Byun HW, Kim YS, et al. A case of disseminated coccidioidomycosis involving lung and skin in patient with diabetes mellitus and iatrogenic cushings syndrome. Tuberc Respir Dis. 2005. 58:399–403.4. Lim G, Woo J, Chung YT, Uh ST, Park CS. A case of pulmonary coccidiodomycosis. Tuberc Respir Dis. 1990. 37:440–444.5. Yang HS, Lee J, Lim CM, Lee SD, Koh Y, Kim WS, et al. A case of coccidioidomycosis manifested as solitary pulmonary nodule. Tuberc Respir Dis. 1999. 46:266–272.6. Shin JS, Lee IS, Shin C, Kim A. Pulmonary coccidioidomycosis diagnosed in an immigrant. Tuberc Respir Dis. 2001. 51:448–452.7. Sinn DH, Kwon YS, Choi SY, Chang WI, Park MK, Han J, et al. A case of pulmonary coccidioidomycosis mimicking lung cancer. Korean J Med. 2005. 69:419–423.8. Kim JH, Hur GY, Jung KH, Jung HC, Park DW, Lee SY, et al. Disseminated coccidioidomycosis presenting with miliary nodules. Tuberc Respir Dis. 2006. 60:97–101.9. Lee JE, Kim HJ, Cho YJ, Joh JS, Han SK, Shim YS, et al. A case of pulmonary coccidioidomycosis that was misdiagnosed as tuberculoma and a review of the reported cases in Korea. Korean J Med. 2007. 72:S206–S210.10. Davies SF, Sarosi GA. Fungal infection of the lung. The big 3--histoplasmosis, blastomycosis, coccidioidomycosis. Postgrad Med. 1983. 73:242–251.11. Chiller TM, Galgiani JN, Stevens DA. Coccidioidomycosis. Infect Dis Clin North Am. 2003. 17:41–57.12. Galgiani JN. Coccidioidomycosis: a regional disease of national importance. Rethinking approaches for control. Ann Intern Med. 1999. 130:293–300.13. Desai SA, Minai OA, Gordon SM, O'Neil B, Wiedemann HP, Arroliga AC. Coccidioidomycosis in non-endemic areas: a case series. Respir Med. 2001. 95:305–309.14. Koepke A, Albus C, Barth A, Bernards P, Schütt-Gerowitt H, Allolio B. Coccidioidomycosis: differential diagnosis of lung infiltrates with peripheral eosinophilia. Dtsch Med Wochenschr. 1989. 114:218–221.15. Kuipers S, Pannekoek BJ, Schellekens H. Pulmonary infection with Coccidioides immitis. Ned Tijdschr Geneeskd. 1996. 140:500–502.
