A Case of Severe Aortic Valve Regurgitation Caused by an Ascending Aortic Aneurysm in a Young Patient With Autosomal Dominant Polycystic Kidney Disease and Normal Renal Function
- Affiliations
-
- 1Regional Cardiovascular Center, Division of Cardiology, Department of Internal Medicine, Chungbuk National University School of Medicine, Cheongju, Korea. drcorazon@hanmail.net
- 2Department of Pathology, Chungbuk National University School of Medicine, Cheongju, Korea.
- 3Department of Pathology, College of Medicine, Seoul National University, Seoul, Korea.
- 4Department of Thoracic and Cardiovascular Surgery, College of Medicine, Seoul National University, Seoul, Korea.
- KMID: 1826389
- DOI: http://doi.org/10.4070/kcj.2012.42.2.136
Abstract
- Aortic aneurysm is one several well-known cardiovascular complications in patients with autosomal dominant polycystic kidney disease (ADPCKD). Commonly affected site of aortic aneurysm and its related dissection in ADPCKD is abdominal aorta. Long standing hypertension, haemodialysis, old age are closely related with discovering of aortic aneurysm and dissection in ADPCKD. However, thoracic aortic aneurysms and its related severe aortic regurgitations (ARs) are rare in younger patients suffering from ADPCKD, especially ones who have normal renal function. Here, we report a case involving a 27-year-old Asian male patient with severe AR due to an ascending aneurysm of the thoracic aorta associated with ADPCKD. The patient had normal renal function without Marfan's habitus. The AR and thoracic aortic aneurysm were corrected surgically.
MeSH Terms
Figure
-

Fig. 1 Chest X-ray of the patient. Mild cardiomegaly without pulmonary congestion was observed.
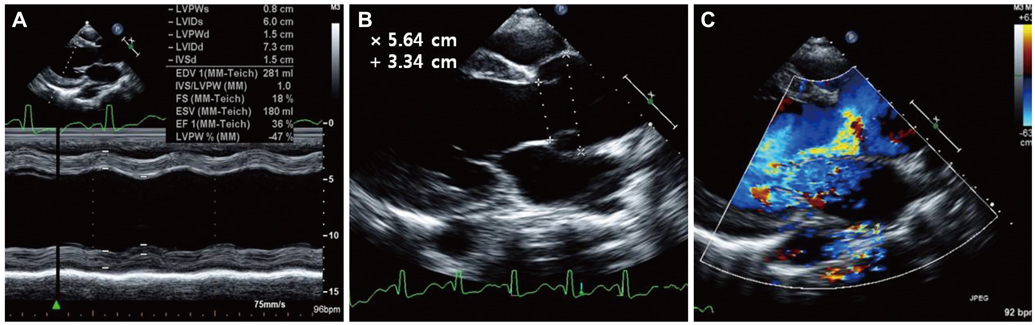
Fig. 2 Echocardiographic findings for the patient. A: left ventricular enlargement and systolic dysfunction was evident. B: markedly dilated aortic valve orifice and ascending thoracic aorta. C: severe aortic valve regurgitation was noticed on doppler echocardiography.
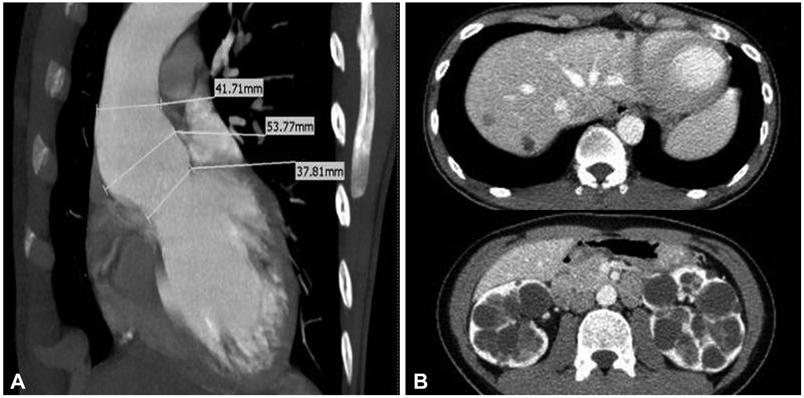
Fig. 3 Cardiac and abdominopelvic CT of the patient. A: dilated ascending thoracic aorta on cardiac CT. B: multiple sized cysts in liver and kidneys were compatible to autosomal dominant poly cystic kidney disease.

Fig. 4 Pathologic finding of excised aortic tissue. A: cystic medial necrosis, which is defined as mucoid material accumulation, was noticed in the aortic media (×200, H & E staining). B: the resected aorta showed medionecrosis of smooth muscle cells, change in muscle cell orientation, and elastic fragmentation (×200, elastic fiber staining). H & E: hematoxylin and eosin.
Cited by 1 articles
-
Multiple Cardiovascular Manifestations in a Patient with Autosomal Dominant Polycystic Kidney Disease
Young Ran Kang, Jong-Hwa Ahn, Kye Hwan Kim, Young Min Choi, Jungwoo Choi, Jeong Rang Park
J Cardiovasc Ultrasound. 2014;22(3):144-147. doi: 10.4250/jcu.2014.22.3.144.
Reference
-
1. Matthias Bechtel JF, Noack F, Sayk F, Erasmi AW, Bartels C, Sievers HH. Histopathological grading of ascending aortic aneurysm: comparison of patients with bicuspid versus tricuspid aortic valve. J Heart Valve Dis. 2003. 12:54–59.2. Gabow PA. Autosomal dominant polycystic kidney disease. N Engl J Med. 1993. 329:332–342.3. Torres VE, Harris PC, Pirson Y. Autosomal dominant polycystic kidney disease. Lancet. 2007. 369:1287–1301.4. Takagi H, Umemoto T. Matrix metalloproteinases synthesized in autosomal dominant polycystic kidney disease play a role in development of a concurrent abdominal aortic aneurysm. Med Hypotheses. 2005. 64:778–781.5. Leier CV, Baker PB, Kilman JW, Wooley CF. Cardiovascular abnormalities associated with adult polycystic kidney disease. Ann Intern Med. 1984. 100:683–688.6. Fick GM, Johnson AM, Hammond WS, Gabow PA. Causes of death in autosomal dominant polycystic kidney disease. J Am Soc Nephrol. 1995. 5:2048–2056.7. Takagi H, Umemoto T. Abdominal aortic aneurysm and autosomal-dominant polycystic kidney disease. Kidney Int. 2005. 67:376.8. Kato A, Takita T, Furuhashi M, Maruyama Y, Hishida A. Abdominal aortic aneurysms in hemodialysis patients with autosomal dominant polycystic kidney disease. Nephron. 2001. 88:185–186.9. Nacasch N, Werner M, Golan E, Korzets Z. Arterial dissections in autosomal dominant polycystic kidney disease-chance association or part of the disease spectrum? Clin Nephrol. 2010. 73:478–481.10. Iglesias CG, Torres VE, Offord KP, Holley KE, Beard CM, Kurland LT. Epidemiology of adult polycystic kidney disease. Olmsted County. Minnesota: 1935-1980. Am J Kidney Dis. 1983. 2:630–639.11. Vanmaele R, Witbreuk M, De Broe M, Van Schil P, Lins R. Abdominal aortic aneurysm and polycystic kidneys. Nephron. 1995. 69:107–108.12. Moon J, Lee SH, Yang WI, Ko YG, Han WK, Jang Y. Fatal renal bleeding in a patient treated with aggressive antithrombotic therapy after recurrent coronary stent thrombosis. Korean Circ J. 2010. 40:348–351.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Dissection in Marfan Syndrome with Ascending Aortic Aneurysm
- A Case of Ascending Aortic Aneurysm Associated with Congenital Bicuspid Aortic Valve
- A Case of Non ST Elevation Myocardial Infarction by Coronary Artery Focal Spasm in a Patient with Autosomal Dominant Polycystic Kidney Disease
- Aortic Valve Sparing Operations: A Review
- Multiple Cardiovascular Manifestations in a Patient with Autosomal Dominant Polycystic Kidney Disease
