Risk Factors Associated with Delayed Traumatic Intraparenchymal Hemorrhage
- Affiliations
-
- 1Department of Radiology, Hanyang University Medical Center, Seoul, Korea.
- 2Department of Neurosurgery, Hanyang University Medical Center, Seoul, Korea. tdy815@hanmail.net
- KMID: 1814436
- DOI: http://doi.org/10.13004/jknts.2008.4.1.8
Abstract
OBJECTIVE
Delayed hemorrhage progression is one of the most common causes of neurologic deterioration after traumatic brain injury (TBI). We herein analyzed the risk factors related to the delayed hemorrhage progression in traumatic intraparenchymal hemorrhage (IPH) or cerebral contusion.
METHODS
A retrospective investigation was performed on selected 105 TBI patients with IPH or cerebral contusion associated with other types of intracranial hematoma during the last 2 years. Clinical features regarding neurologic grade, time intervals from the initial injury to delayed traumatic IPH, and initial computed tomographic (CT) findings including midline shifting, cisternal effacement, and location were studied. For majority of patients, follow-up CT scans were checked at 8, 24, 72 hours after trauma, except patients with sudden neurologic deterioration.
RESULTS
Among 105 patients with traumatic IPH, 49 patients showed hemorrhage progression. Traumatic subarachnoid hemorrhage (SAH) is the most commonly accompanied hemorrhage with IPH patients. The most frequent location of hemorrhage progression was the frontal lobe, and time interval for identifying delayed IPH was within the first 8 hours in 31 patients (63%). There was statistically significant correlation between IPH progression and presence of SAH (p=0.03) and effacement of cisterns (p<0.0001).
CONCLUSION
We should closely observe traumatic IPH or cerebral contusion patients who have initial CT findings of traumatic SAH and cisternal effacement. It is primarily because hemorrhage progression is very likely to occur in this patient group. Although we could not draw conclusion regarding time for CT surveillance, bed-side clinical monitoring is of utmost importance.
Keyword
MeSH Terms
Figure
-

FIGURE 1 A 49-year-old man is admitted for headache following slip down. Initial brain computed tomogram shows subarachnoid hemorrhage on the right sylvian fissure and minimal contusion on the right temporal area (A). A computed tomographic angiography do not disclose any vascular lesion (B). Twelve hours later, he became stuporous and follow-up computed tomography reveals huge (Intraparenchymal hemorrhage on the right temporal avea cc).
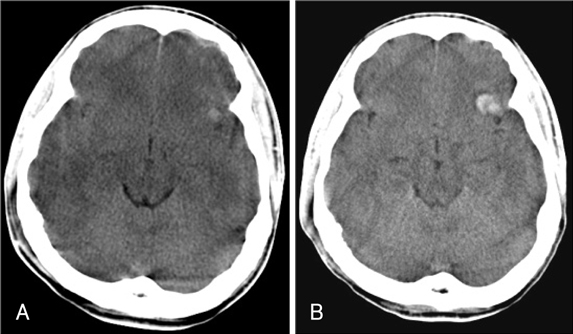
FIGURE 2 A 48-year-old man is admitted to our department after in-car collision accident. Initial computed tomography shows small contusion on the left sylvian and the frontal lobe. Prominent cisternal effacement is also noted on both sylvian fissures and basal cisterns (A). According to the designated schedule, follow-up brain CT is performed at 24 hours later and it shows minimally increased hemorrhage on the left sylvian area (B).
Reference
-
1. Brown FD, Mullan S, Duda EE. Delayed traumatic intracerebral hematomas. Report of three cases. J Neurosurg. 1978; 48:1019–1022.2. Bullock R, Zauner A, Woodward JJ, Myseros J, Choi SC, Ward JD, et al. Factors affecting excitatory amino acid release following severe human head injury. J Neurosurg. 1998; 89:507–518.
Article3. Chang EF, Meeker M, Holland MC. Acute traumatic intraparenchymal hemorrhage: risk factors for progression in the early post-injury period. Neurosurgery. 2006; 58:647–656.
Article4. Chieregato A, Fainardi E, Morselli-Labate AM, Antonelli V, Compagnone C, Targa L, et al. Factors associated with neurological outcome and lesion progression in traumatic subarachnoid hemorrhage patients. Neurosurgery. 2005; 56:671–680.
Article5. Chieregato A, Fainardi E, Servadei F, Tanfani A, Pugliese G, Pascarella R, et al. Centrifugal distribution of regional cerebral blood flow and its time course in traumatic intracerebral hematomas. J Neurotrauma. 2004; 21:655–666.
Article6. Diaz FG, Yock DH Jr, Larson D, Rockswold GL. Early diagnosis of delayed posttraumatic intracerebral hematomas. J Neurosurg. 1979; 50:217–223.
Article7. Elsner H, Rigamonti D, Corradino G, Schlegel R Jr, Joslyn J. Delayed traumatic intracerebral hematomas: "Spät-Apoplexie". Report of two cases. J Neurosurg. 1990; 72:813–815.8. French BN, Dublin AB. The value of computerized tomography in the management of 1000 consecutive head injuries. Surg Neurol. 1977; 7:171–183.9. Fukamachi A, Kohno K, Nagaseki Y, Misumi S, Kunimine H, Wakao T. The incidence of delayed traumatic intracerebral hematoma with extradural hemorrhages. J Trauma. 1985; 25:145–149.
Article10. Kazui S, Naritomi H, Yamamoto H, Sawada T, Yamaguchi T. Enlargement of spontaneous intracerebral hemorrhage. Incidence and time course. Stroke. 1996; 27:1783–1787.11. Lee JH, Martin NA, Alsina G, McArthur DL, Zaucha K, Hovda DA, et al. Hemodynamically significant cerebral vasospasm and outcome after head injury: a prospective study. J Neurosurg. 1997; 87:221–233.
Article12. Lobato RD, Gomez PA, Alday R, Rivas JJ, Dominguez J, Cabrera A, et al. Sequential computerized tomography changes and related final outcome in severe head injury patients. Acta Neurochir (Wien). 1997; 139:385–391.
Article13. Martin NA, Doberstein C, Zane C, Caron MJ, Thomas K, Becker DP. Posttraumatic cerebral arterial spasm: transcranial Doppler ultrasound, cerebral blood flow, and angiographic findings. J Neurosurg. 1992; 77:575–583.
Article14. McIntosh TK. Novel pharmacological therapies in the treatment of experimental traumatic brain injury: a review. J Neurotrauma. 1993; 10:215–261.15. Oertel M, Kelly DF, McArthur D, Boscardin WJ, Glenn TC, Lee JH, et al. Progressive hemorrhage after head trauma: predictors and consequences of the evolving injury. J Neurosurg. 2002; 96:109–116.
Article16. Poon WS, Rehman SU, Poon CY, Li AK. Traumatic extradural hematoma of delayed onset is not a rarity. Neurosurgery. 1992; 30:681–686.
Article17. Schröder ML, Muizelaar JP, Bullock MR, Salvant JB, Povlishock JT. Focal ischemia due to traumatic contusions documented by stable xenon-CT and ultrastructural studies. J Neurosurg. 1995; 82:966–971.
Article18. Servadei F, Antonelli V, Giuliani G, Fainardi E, Chieregato A, Targa L. Evolving lesions in traumatic subarachnoid hemorrhage: prospective study of 110 patients with emphasis on the role of ICP monitoring. Acta Neurochir Suppl. 2002; 81:81–82.
Article19. Servadei F, Nanni A, Nasi MT, Zappi D, Vergoni G, Giuliani G, et al. Evolving brain lesions in the first 12 hours after head injury: analysis of 37 comatose patients. Neurosurgery. 1995; 37:899–907.20. von Oettingen G, Bergholt B, Gyldensted C, Astrup J. Blood flow and ischemia within traumatic cerebral contusions. Neurosurgery. 2002; 50:781–790.
Article21. Zauner A, Bullock R. The role of excitatory amino acids in severe brain trauma: opportunities for therapy: a review. J Neurotrauma. 1995; 12:547–554.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Assessment of the Clinical and the Radiological Prognostic Factors that Determine the Management of a Delayed, Traumatic, Intraparenchymal Hemorrhage (DTIPH)
- A Clinical Analysis of Delayed Traumatic Intracerebral Hemorrhage
- Contralateral Intraparenchymal Hemorrhage Following Aneurysmal Clipping
- Delayed Traumatic Intracerebral Hemorrhage
- Delayed Rupture of Traumatic Intracranial Aneurysm Developed by Minor Head Trauma
