Infect Chemother.
2012 Dec;44(6):465-468. 10.3947/ic.2012.44.6.465.
Multicystic Mass Infection in the Subcutaneous Tissue around Joint Developed by Aspergillus in a Liver Transplant Patient
- Affiliations
-
- 1Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea. shhan74@yuhs.ac
- 2AIDS Research Institute, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 1806934
- DOI: http://doi.org/10.3947/ic.2012.44.6.465
Abstract
- Invasive aspergillosis can be occured in immune-compromised patients with hematopoietic stem cell transplantation, solid organ transplantation and prolonged neutropenia. The major area of invasive aspergillosis involves the sinopulmonary tract but can occur around the joint areas rarely. A 72-year-old man, who had received a liver transplant 6 years earlier, presented with a mass lesion around the right knee joint that developed 3 year earlier. Knee MRI revealed a multicystic subcutaneous mass around the knee joint. An excision was performed, and many fungal hyphae that were morphologically most consistent with Aspergillus spp. were observed in tissue. After amphotericin B therapy for 2 weeks, the patient did not show any evidence of a recurrence of invasive aspergillosis for 15 months. As Aspergillus spp. can cause a range of infections in solid organ transplants, invasive aspergillosis must be considered in patients with a recurrent cystic mass lesion.
Keyword
MeSH Terms
Figure
-
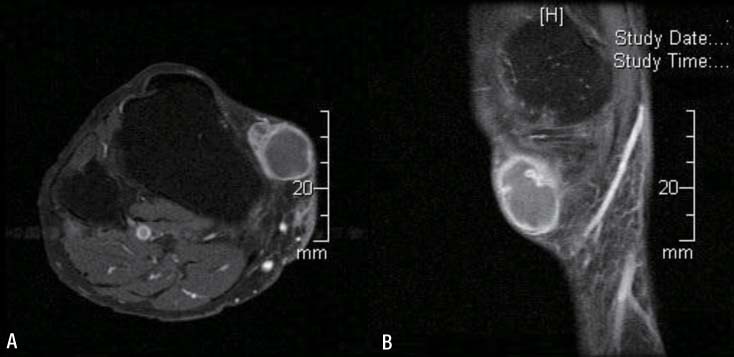
Figure 1 Findings of the right lower extremity MRI in (A) coronal view (B) sagittal view show the 2.7×1.9×3.1 cm sized multicystic mass at the anteromedial aspect of the proximal lower leg (Arrow).
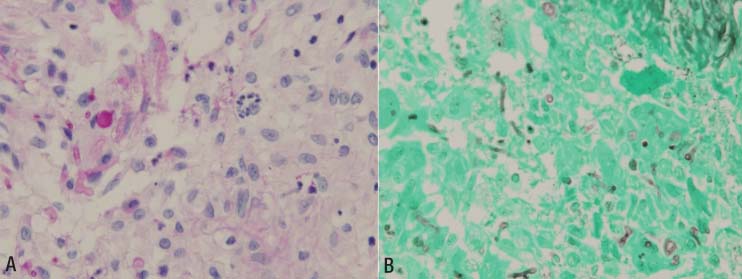
Figure 2 Pathologic examination of the excisional mass (A) D-PAS and (B) GMS stain showing acute suppurative inflammation with giant cells (arrow) and the presence of many fungal hyphae (arrow, that were morphologically most consistent with Aspergillus spp.
Reference
-
1. Segal BH. Aspergillosis. N Engl J Med. 2009. 360:1870–1884.
Article2. Golmia R, Bello I, Marra A, Hamerschlak N, Osawa A, Scheinberg M. Aspergillus fumigatus joint infection: a review. Semin Arthritis Rheum. 2011. 40:580–584.
Article3. Kim T, Lee SR, Cho OH, Park KH, Oh R, Lee SO, Kim YS, Woo JH, Kim MN, Choi SH. A case of septic hip arthritis caused by aspergillus fumigatus in a liver transplantation recipient. Infect Chemother. 2008. 40:170–174.
Article4. Austin KS, Testa NN, Luntz RK, Greene JB, Smiles S. Aspergillus infection of total knee arthroplasty presenting as a popliteal cyst. Case report and review of the literature. J Arthroplasty. 1992. 7:311–314.
Article5. Upton A, Kirby KA, Carpenter P, Boeckh M, Marr KA. Invasive aspergillosis following hematopoietic cell transplantation: outcomes and prognostic factors associated with mortality. Clin Infect Dis. 2007. 44:531–540.
Article6. Pfaller MA, Diekema DJ. Epidemiology of invasive candidiasis: a persistent public health problem. Clin Microbiol Rev. 2007. 20:133–163.
Article7. Salman N, Törün SH, Budan B, Somer A. Invasive aspergillosis in hematopoietic stem cell and solid organ transplantation. Expert Rev Anti Infect Ther. 2011. 9:307–315.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Necrotizing Fasciitis following Liver Transplantation
- A Case of Septic Hip Arthritis Caused by Aspergillus fumigatus in a Liver Transplant Recipient
- Simultaneous Lung and Liver Aspergillus in a Kidney Transplant Recipient
- Treatment for Multiple Aspergillus Spondylitis Including a Hip Joint
- Iatrogenic Subcutaneous Aspergillosis in a Patient with Lumbar Spondylitis Treated with Ketoconazole
