Endovascular stenting of the inferior vena cava in a patient with Budd-Chiari syndrome and main hepatic vein thrombosis: a case report
- Affiliations
-
- 1Department of Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. shwang@amc.seoul.kr
- 2Department of Diagnostic Imaging, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- 3Department of Gastroenterology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- KMID: 1802238
- DOI: http://doi.org/10.14701/kjhbps.2015.19.1.35
Abstract
- Endovascular stenting is accepted as an effective treatment for patients with Budd-Chiari syndrome (BCS). We herein present a case of successful endovascular treatment. A 46-year-old woman, who was followed up for 10 years after a diagnosis of BCS, showed progression progressive of liver cirrhosis and deterioration deteriorated of liver function. Three main hepatic veins were thrombosed with complete occlusion of the suprahepatic of the inferior vena cava (IVC); thus, hepatic venous blood flow was draining into the inferior right hepatic veins through the intrahepatic collaterals and passed passing through the subcutaneous venous collaterals. She underwent endovascular stenting of the IVC for palliation. A septoplasty needle was passed through the occluded IVC through into the internal jugular vein access and then to access the femoral vein using a snare wire. Severe elastic recoiling was observed after balloon dilatation; thus, a 28x80 mm stenting was done inserted across the occlusion, and repeat double ballooning was performed. The final venogram shows showed restored IVC inflow. The patient began to lose body weight 1 day after stenting, and edema disappeared within 1 week. She is was doing well at the 6 month follow-up visit with nearly normal liver function and marked resolution of cutaneous venous engorgement. In conclusion, endovascular stenting appeared to be an effective treatment to alleviate portal pressure and to prevent BCS-associated complications; thus, endovascular stenting should be considered before marked hepatic vein stenosis or complete occlusion occurs in patients with BCS.
MeSH Terms
Figure
-
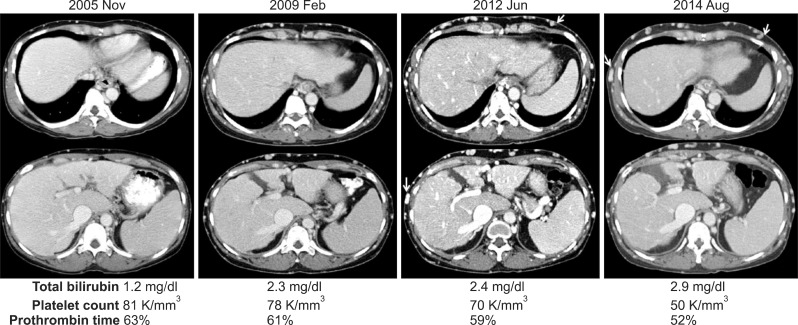
Fig. 1 Clinical sequence in a patient with Budd-Chiari syndrome and a 10 year follow-up. Computed tomography image shows progressive advanced liver cirrhosis with prominent development of subcutaneous venous collaterals (arrows). Liver function and coagulation profiles deteriorated concurrently over time.
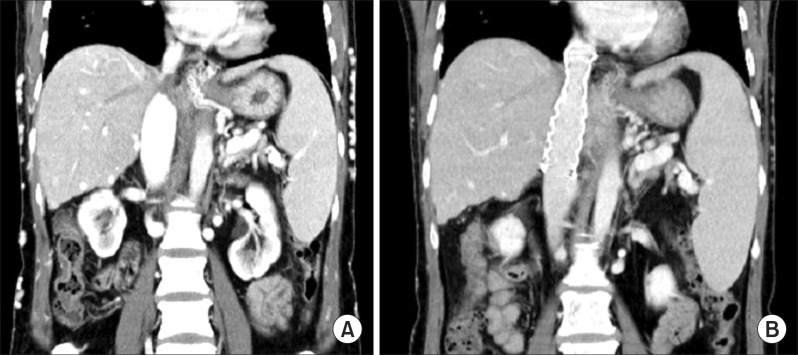
Fig. 2 Computed tomography images revealing the status of the retrohepatic inferior vena cava before (A) and after endovascular stenting (B).
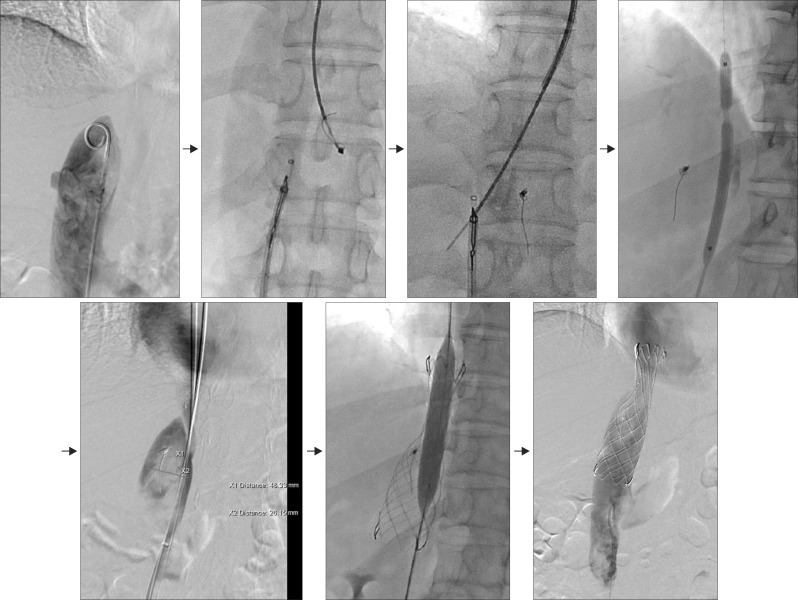
Fig. 3 Interventional endovascular stenting procedure for the inferior vena cava. The rendezvous technique was applied by assessing the internal jugular vein and femoral vein. A 28×80-mm sized stent was placed, and repeat double ballooning was performed.
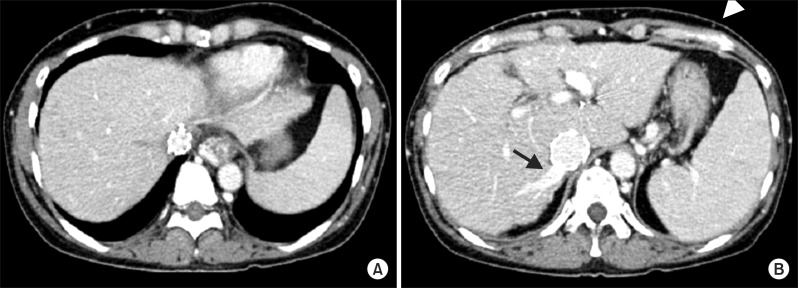
Fig. 4 Follow-up computed tomography image at 3 months shows complete thrombosis of the three main hepatic veins (A), intrahepatic collateral flow drainage through the right inferior hepatic vein (arrow), and collapsed subcutaneous collateral veins (arrow head) (B).
Reference
-
1. Okuda K, Kage M, Shrestha SM. Proposal of a new nomenclature for Budd-Chiari syndrome: hepatic vein thrombosis versus thrombosis of the inferior vena cava at its hepatic portion. Hepatology. 1998; 28:1191–1198. PMID: 9794901.
Article2. Cazals-Hatem D, Vilgrain V, Genin P, Denninger MH, Durand F, Belghiti J, et al. Arterial and portal circulation and parenchymal changes in Budd-Chiari syndrome: a study in 17 explanted livers. Hepatology. 2003; 37:510–519. PMID: 12601347.
Article3. Janssen HL, Garcia-Pagan JC, Elias E, Mentha G, Hadengue A, Valla DC. European Group for the Study of Vascular Disorders of the Liver. Budd-Chiari syndrome: a review by an expert panel. J Hepatol. 2003; 38:364–371. PMID: 12586305.
Article4. Xue H, Li YC, Shakya P, Palikhe M, Jha RK. The role of intravascular intervention in the management of Budd-Chiari syndrome. Dig Dis Sci. 2010; 55:2659–2663. PMID: 20035404.
Article5. Sang HF, Li XQ. Endovascular treatment of Budd-Chiari syndrome with hepatic vein obstruction in China. J Laparoendosc Adv Surg Tech A. 2014; 24:846–851. PMID: 25495251.
Article6. Darwish Murad S, Plessier A, Hernandez-Guerra M, Fabris F, Eapen CE, Bahr MJ, et al. EN-Vie (European Network for Vascular Disorders of the Liver). Etiology, management, and outcome of the Budd-Chiari syndrome. Ann Intern Med. 2009; 151:167–175. PMID: 19652186.
Article7. Aydinli M, Bayraktar Y. Budd-Chiari syndrome: etiology, pathogenesis and diagnosis. World J Gastroenterol. 2007; 13:2693–2696. PMID: 17569137.
Article8. Beckett D, Olliff S. Interventional radiology in the management of Budd Chiari syndrome. Cardiovasc Intervent Radiol. 2008; 31:839–847. PMID: 18214592.
Article9. Parker R. Role of transjugular intrahepatic portosystemic shunt in the management of portal hypertension. Clin Liver Dis. 2014; 18:319–334. PMID: 24679497.
Article10. Wei X, Hao X, Da-Hai Y, Mao-Heng Z, Qing-Qiao Z, Yu-Ming G. Analysis of interventional treatments of Budd-Chiari Syndrome and the related complications: a study of 1006 cases. Panminerva Med. 2013; 55:371–376. PMID: 24172863.11. Eapen CE, Velissaris D, Heydtmann M, Gunson B, Olliff S, Elias E. Favourable medium term outcome following hepatic vein recanalisation and/or transjugular intrahepatic portosystemic shunt for Budd Chiari syndrome. Gut. 2006; 55:878–884. PMID: 16174658.
Article12. Darwish Murad S, Valla DC, de Groen PC, Zeitoun G, Hopmans JA, Haagsma EB, et al. Determinants of survival and the effect of portosystemic shunting in patients with Budd-Chiari syndrome. Hepatology. 2004; 39:500–508. PMID: 14768004.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Budd Chiari Syndrome Caused by Membraneous Obstruction of Suprahepatic Inferior Vena Cava
- Mesoatrial Shunt Operation for Treatment of Budd-Chiari Syndrome: A case report
- Hepatoblastoma with budd-chiari syndrome in child: a case report
- Budd-Chiari syndrome associated with diaphragmatic hernia: A case report
- Balloon Angioplasty for Budd-Chiari Syndrome Resulting from Primary Repair of an Inferior Vena Cava Injury
