Differential Diagnosis of Lemierre's Syndrome in a Patient with Acute Paresis of the Abducens and Oculomotor Nerves
- Affiliations
-
- 1Department of Radiology, Cantonal Hospital Winterthur, Winterthur, Switzerland. andreas.gutzeit@ksw.ch
- 2Department of Radiology, University Salzburg, Salzburg, Austria.
- 3Department of Medicine, Cantonal Hospital Winterthur, Winterthur, Switzerland.
- 4Department of Ophthalmology, Cantonal Hospital Winterthur, Winterthur, Switzerland.
- 5Department of Radiology, University Basel, Basel, Switzerland.
- 6Department of Neurology, Cantonal Hospital Winterthur, Winterthur, Switzerland.
- 7Department of Neurosurgery, Cantonal Hospital Winterthur, Winterthur, Switzerland.
- KMID: 1798063
- DOI: http://doi.org/10.3341/kjo.2013.27.3.219
Abstract
- Lemierre's syndrome is characterized by anaerobic septicemia, internal jugular vein thrombosis, and septic emboli associated with infections of the head and neck. We describe an unusual and clinically confusing case of a young woman with an acute paresis of the abducens nerve and partial paresis of the right oculomotor nerve. After an extensive imaging diagnostic procedure, we also documented a peritonsillar abscess and various types of thromboses in intracranial and extracranial veins. Furthermore, we found brain and lung abscesses, which led us to establish the diagnosis of Lemierre's syndrome. Despite intensive anti-coagulation and antibiotic therapy, the patient developed a mycotic aneurysm in the right internal carotid artery directly adjacent to the previously thrombosed cavernous sinus. In summary, we were able to confirm that Lemierre's syndrome may occur in conjunction with uncharacteristic symptoms. Due to the sometimes confusing clinical symptoms as well as clinical and radiological specialties, we had to work on an interdisciplinary basis to minimize the delay prior to establishing the diagnosis and therapy.
MeSH Terms
Figure
-

Fig. 1 The patient presented with clinical signs of oculomotor nerve paresis on the right side. As a result, she had a drooping right eyelid. She also demonstrated exophthalmos on the right side.

Fig. 2 The patient presented with paresis of the abducens nerve in the right eye when looking to the right.
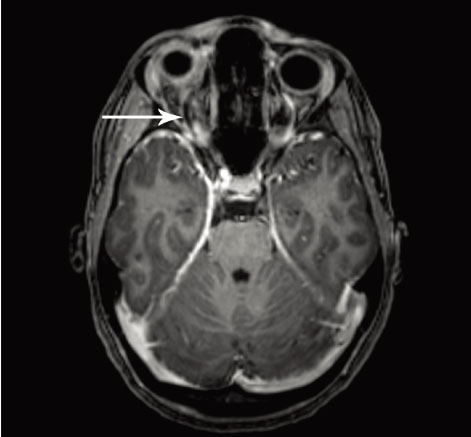
Fig. 3 Coronal view on 3-D T1-weighted magnetic resonance imaging after administration of gadolinium reveals the cavernous sinus with thrombosis on both sides, but more pronounced on the right side (arrow).
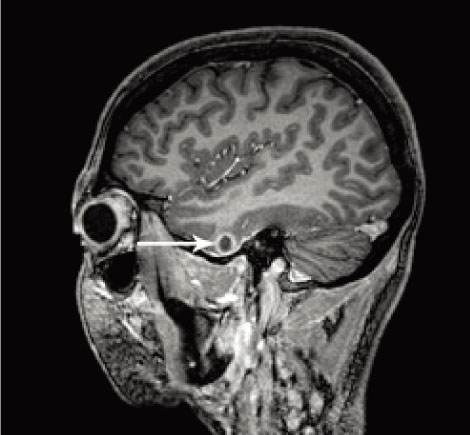
Fig. 4 Axial view on a 3-D T1-weighted sequence after administration of gadolinium reveals a thrombosis in the superior ophthalmic vein on the right side (arrow).
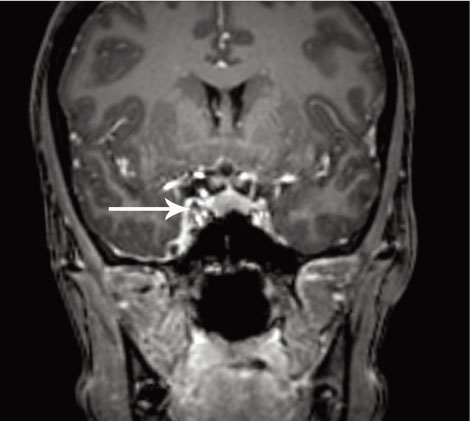
Fig. 5 Intra-axial brain abscess in the right temporal lobe, which worsened rapidly despite treatment with a broad-spectrum antibiotic (arrow).
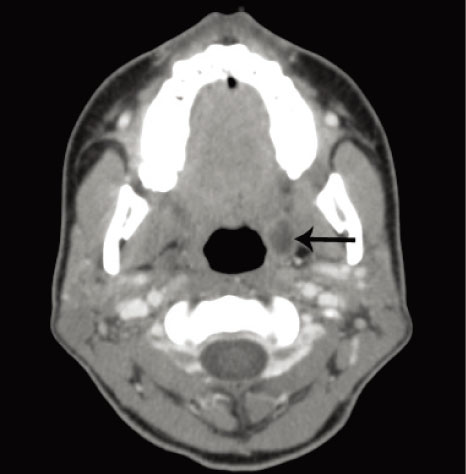
Fig. 6 Computed tomography of the neck shows a clearly delineated tonsillary abscess on the left side with a maximum diameter of 1.3 cm.
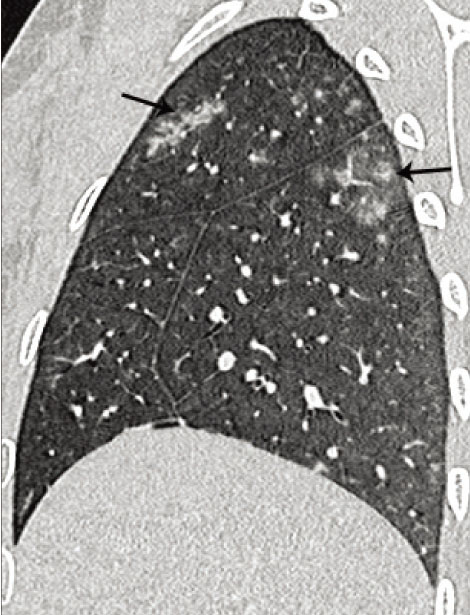
Fig. 7 Note the numerous septic emboli in both lungs. The emboli are clearly seen along the bronchovascular bundle.

Fig. 8 In addition to known venous thrombi, the magnetic resonance angiography revealed a recent mycotic aneurysm in the right internal carotid artery, directly adjacent to the previously thrombosed cavernous sinus on the right side.
Reference
-
1. Lemierre A. On certain septicaemias due to anaerobic organisms. Lancet. 1936. 227:701–703.2. Courmont P, Cade A. Sur une septico-pyohemie de l'homme simulant la peste et causee par un streptobacille anaerobie. Arch Med Exp Anat Pathol. 1900. 4:17–28.3. Shannon GW, Ellis CV, Stepp WP. Oropharyngeal bacteroides melaninogenicus infection with septicemia: Lemierre's syndrome. J Fam Pract. 1983. 16:159–160. 1631664. Riordan T, Wilson M. Lemierre's syndrome: more than a historical curiosa. Postgrad Med J. 2004. 80:328–334.5. Kos S, Kraft M, Michot MP. Lemierre syndrome: diagnosis with multimodal imaging. Rofo. 2007. 179:1198–1199.6. Chirinos JA, Lichtstein DM, Garcia J, Tamariz LJ. The evolution of Lemierre syndrome: report of 2 cases and review of the literature. Medicine (Baltimore). 2002. 81:458–465.7. Jankowich M, El-Sameed YA, Abu-Hijleh M. A 21-year-old man with fever and sore throat rapidly progressive to hemoptysis and respiratory failure: diagnosis: Lemierre syndrome with Fusobacterium necrophorum sepsis. Chest. 2007. 132:1706–1709.8. Weeks DF, Katz DS, Saxon P, Kubal WS. Lemierre syndrome: report of five new cases and literature review. Emerg Radiol. 2010. 17:323–328.9. Carlson ER, Bergamo DF, Coccia CT. Lemierre's syndrome: two cases of a forgotten disease. J Oral Maxillofac Surg. 1994. 52:74–78.10. Syed MI, Baring D, Addidle M, et al. Lemierre syndrome: two cases and a review. Laryngoscope. 2007. 117:1605–1610.11. Beldman TF, Teunisse HA, Schouten TJ. Septic arthritis of the hip by Fusobacterium necrophorum after tonsillectomy: a form of Lemierre syndrome? Eur J Pediatr. 1997. 156:856–857.12. Leugers CM, Clover R. Lemierre syndrome: postanginal sepsis. J Am Board Fam Pract. 1995. 8:384–391.13. Bentham JR, Pollard AJ, Milford CA, et al. Cerebral infarct and meningitis secondary to Lemierre's syndrome. Pediatr Neurol. 2004. 30:281–283.14. Agarwal R, Arunachalam PS, Bosman DA. Lemierre's syndrome: a complication of acute oropharyngitis. J Laryngol Otol. 2000. 114:545–547.15. Peer Mohamed B, Carr L. Neurological complications in two children with Lemierre syndrome. Dev Med Child Neurol. 2010. 52:779–781.16. Jones C, Siva TM, Seymour FK, O'Reilly BJ. Lemierre's syndrome presenting with peritonsillar abscess and VIth cranial nerve palsy. J Laryngol Otol. 2006. 120:502–504.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Cystic Abducens Schwannoma without Abducens Paresis : Possible Role of Cisternal Structures in Clinical Manifestation
- A Case of Lemierre Syndrome as a Cause of Revisiting the Emergency Department
- Pituitary Apoplexy Presenting as Isolated Oculomotor Nerve Palsy
- Acute unilateral isolated abducens nerve palsy associated with anti-GM1 immunoglobulin M antibody
- A Case of Lemierre Syndrome Manifests with Persistent Fever and Neck Stiffness Following Acute Oropharyngeal Infection
