Transmasseteric antero-parotid facelift approach for open reduction and internal fixation of condylar fractures
- Affiliations
-
- 1Department of Oral and Maxillofacial Surgery, Wonkwang University School of Dentistry, Iksan, Korea. omschoi@wonkwang.ac.kr
- KMID: 1797846
- DOI: http://doi.org/10.5125/jkaoms.2015.41.3.149
Abstract
- Surgical approaches to the condylar fracture include intraoral, preauricular, submandibular, and retromandibular approaches. Each approach has its own advantages and disadvantages. When a patient needs esthetic results and an intraoral approach is not feasible, the transmasseteric antero-parotid facelift approach is considered. This approach permits direct exposure and allow the surgeon to fixate the fractured unit tangentially. Tangential fixation is critical to osteosynthesis. Disadvantages of the transmasseteric antero-parotid facelift approach include damage to the facial nerve and a longer operation time. However, after the initial learning curve, facial nerve damage can be avoided and operation time may decrease. We report three cases of subcondylar fractures that were treated with a transmasseteric antero-parotid facelift approach. Among these, two cases had trivial complications that were easily overcome. Instead of dissecting through the parotid gland parenchyma, the transmasseteric antero-parotid facelift approach uses transmasseteric dissection and reduces facial nerve damage more than the retromandibular transparotid approach. The esthetic result is superior to that of other approaches.
Figure
-

Fig. 1 A. Outline of a rhytidectomy incision incorporating a preauricular incision in men. The incision extends into the posterior auricular crease, and runs parallel to the hair line for approximately 5 to 6 cm in a posteroinferior direction. B. In women, an endaural incision must be used. The post-auricular incision must be positioned anterior to the auricular crease. Usually, the incision line is anterior to the crease by 2 to 3 mm.

Fig. 2 The skin flap is elevated to expose the anterior edge of the parotid gland.
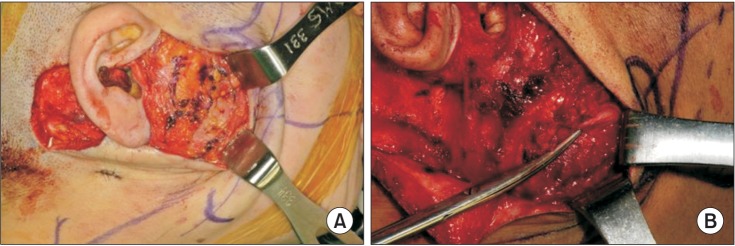
Fig. 3 A. Incision of the subcutaneous musculoaponeurotic system on the anterior edge of the parotid gland exposes the emerging facial nerve. B. The tip of the scissors indicates the buccal branch of the facial nerve.
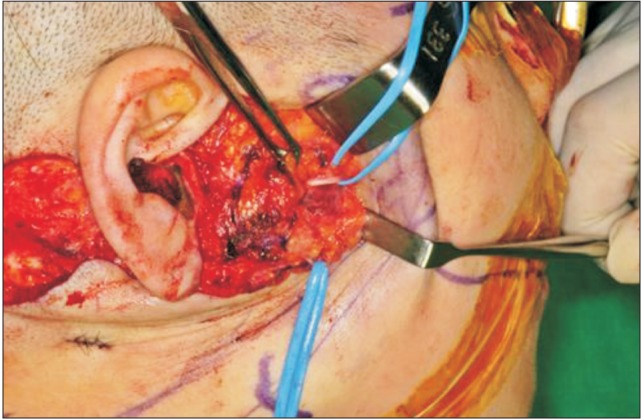
Fig. 4 Retraction of the parotid gland exposes the underlying masseter muscle, and branches of facial nerve are retracted away from the surgical field with the aid of vessel loops. The vessel loops retracted the upper and lower buccal branches.
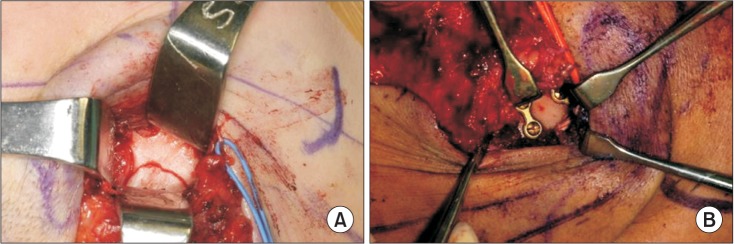
Fig. 5 A. The muscle fibers of the masseter muscle are incised obliquely to expose the fractured site. B. Miniplate fixation was performed after reduction of the fractured site.
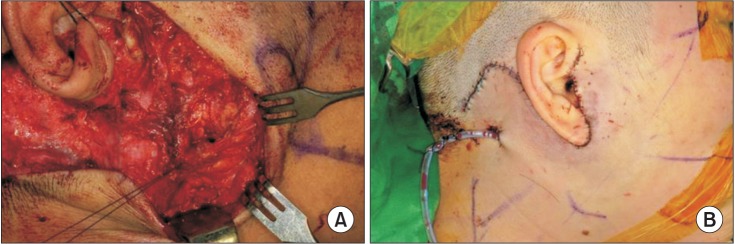
Fig. 6 A. The subcutaneous musculoaponeurotic system layer is closed with 4-0 vicryl. B. The skin flap is closed in two layers; the subdermal layer is closed with 4-0 vicryl and the skin is closed with 5-0 and 6-0 nylon.
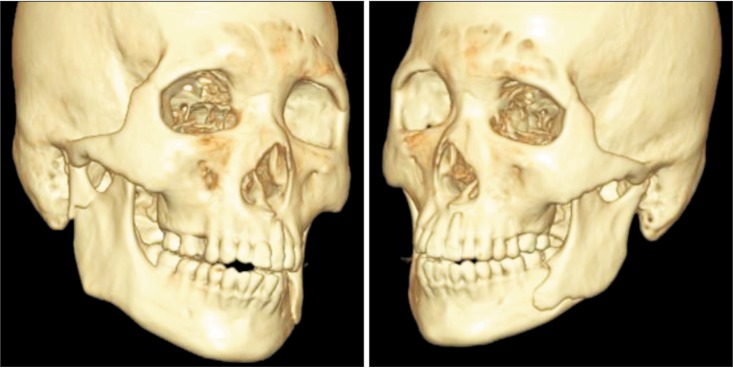
Fig. 7 The patient had a level IV condylar fracture on the right side and a mandibular angle fracture on the left side.

Fig. 8 Postoperative X-ray.

Fig. 9 Good esthetic results were achieved. The facial scar line was inconspicuous on profile and frontal views.
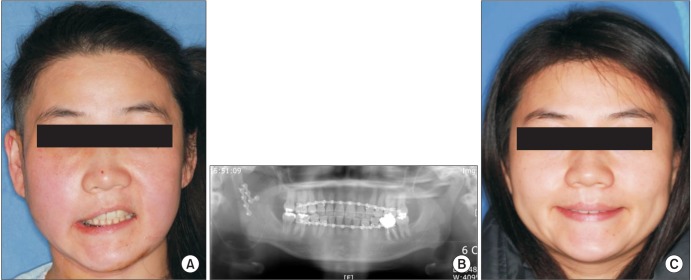
Fig. 10 A. After the operation, paralysis of the upper lip occurred, possibly due to severe retraction of the facial nerve. B. Postoperative panoramic view. C. Nerve function recovered after three months.
Reference
-
1. Divaris M, Blugerman G, Paul MD. Face expressive lifting (FEL): an original surgical concept combined with bipolar radiofrequency. Eur J Plast Surg. 2014; 37:69–76. PMID: 24465090.
Article2. Lindahl L. Condylar fractures of the mandible. I. Classification and relation to age, occlusion, and concomitant injuries of teeth and teeth-supporting structures, and fractures of the mandibular body. Int J Oral Surg. 1977; 6:12–21. PMID: 402318.3. Lee C, Mueller RV, Lee K, Mathes SJ. Endoscopic subcondylar fracture repair: functional, aesthetic, and radiographic outcomes. Plast Reconstr Surg. 1998; 102:1434–1443. discussion 1444-5PMID: 9773997.
Article4. Loukota RA. Endoscopically assisted reduction and fixation of condylar neck/base fractures--The learning curve. Br J Oral Maxillofac Surg. 2006; 44:480–481. PMID: 16423433.
Article5. Salgarelli AC, Anesi A, Bellini P, Pollastri G, Tanza D, Barberini S, et al. How to improve retromandibular transmasseteric anteroparotid approach for mandibular condylar fractures: our clinical experience. Int J Oral Maxillofac Surg. 2013; 42:464–469. PMID: 23395651.
Article6. Manisali M, Amin M, Aghabeigi B, Newman L. Retromandibular approach to the mandibular condyle: a clinical and cadaveric study. Int J Oral Maxillofac Surg. 2003; 32:253–256. PMID: 12767870.
Article7. Widmark G, Bågenholm T, Kahnberg KE, Lindahl L. Open reduction of subcondylar fractures. A study of functional rehabilitation. Int J Oral Maxillofac Surg. 1996; 25:107–111. PMID: 8727580.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Transmasseteric Approach for Open Reduction and Internal Fixation of Mandible Subcondylar Fracture
- Modified high-submandibular appraoch for open reduction and internal fixation of condylar fracture: case series report
- New protocol for simplified reduction and fixation of subcondylar fractures of the mandible: a technical note
- Complications of the retromandibular transparotid approach for low condylar neck and subcondylar fractures: a retrospective study
- Retromandibular approach for open reduction & internal fixation of mandibular condylar neck fracture
